Introduction:
The “hidden” internal root anatomy is the most unpredictable factor of an endodontic treatment, nevertheless the knowledge of the “normal” pulp system and its most frequent variations is basic for clinical success. The goal of root canal therapy is the thorough cleaning and obturation of the entire root canal system.[1]
Hess and Zurcher’s landmark study in 1925 showed the mesial root of the lower first molar and the mesiobuccal root of the upper molars had the most ramifications of any teeth.[2] The incidence of two canals in the mesiobuccal root has been reported to be 18% and 96.1% for maxillary first molar and 58% for maxillary second molars.[3]Of the 140 extracted maxillary first molars, only one tooth showed seven root canals in which three mesiobuccal canals, 3 distobuccal canals, and one palatal canal were identified.[4] The review of cases that had more than 4 canals in maxillary molars is summarized in Table 1.
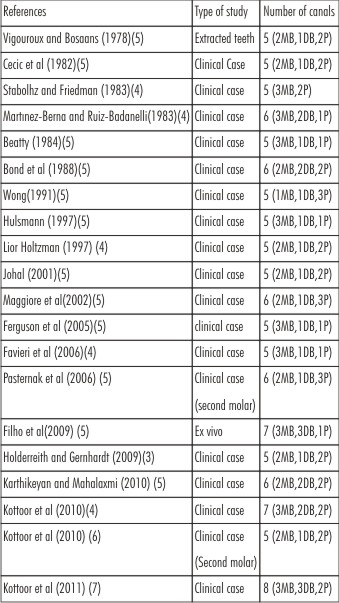 | Table1: Previous Case Reports Of Maxillary Molars Having More Than 4 Canals
 |
The purpose of this case report is to highlight the importance of using SCT in successful endodontic management of a maxillary first molar with three roots and seven canals. This advanced endodontic aid interestingly identified bilateral evidence of multiple canal system in both maxillary first and second molars all in single patient, a rare entity.
Case History:
A healthy 36-year-old man was referred by a private dentist to Department of Conservative Dentistry and Endodontics, Panineeya Mahavidyalaya Institute of Dental Sciences who attempted root canal in the left maxillary first molar #26 .On careful clinical evaluation a diagnosis of irreversible pulpitis with apical periodontitis was made with tooth #26.
A conventional endodontic access opening was already present without any coronal restoration. After rubber dam isolation,the carious tooth structure was removed,the three principal root canals were identified: Mesiobuccal (MB),Distobuccal (DB),and Palatal. On probing with DG 16 endodontic explorer (Hu-Friedy,Chicago,IL) and scrapping calcifications with a spoon excavator, two canal openings in each of the mesiobuccal, distobuccal and palatal root were revealed. During examination with a magnifying loupe, a small haemorrhagic point was noted approximately 3mm from the MB in the palatal direction. The conventional triangular access was modified to a trapezoidal shape to improve access to the additional canals (Figure 1). A nickel-titanium ProTaper series orifice shaper (Denstply Maillefer, Ballaigues, Switzerland) with 17%ethylenediaminetetraacetic acid (Glyde; Denstply Maillefer, Ballaigues, Switzerland) was used to preflare coronal portion of the canals to improve the straight line access. The working length was determined with the help of an apex locator (RootZX;Morita,Tokyo,Japan) and later confirmed using a radiograph (Figure 2). Though, multiple radiographs were taken at different angulations, it did not reveal the number and morphology of the root canal systems.
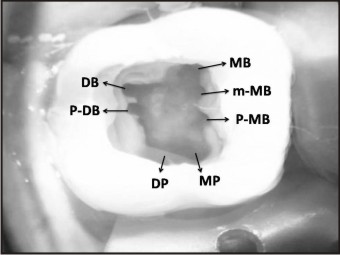 | Figure 1: Access opening showing seven canal orifices (#26)
|
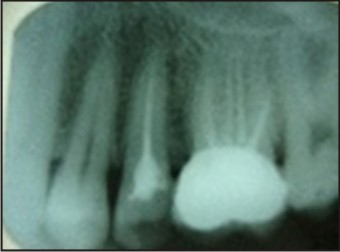
 | Figure 2: Working length radiograph(#26)
|
To confirm this multiple canal morphology of this tooth, dental imaging with Spiral Computer Tomography was planned. Access cavity was sealed with Cavit G (3M ESPE,}3;efeld, Germany) and an informed consent from the patient was obtained. A multislice helical or SCT was performed of maxilla (Sensation 64, Siemens-Somatom Erlangen, Germany) using dental software Dentascan. The tooth in question was focused and its morphology was obtained in transverse, axial and sagittal sections of 0.5mm thickness using 14.10 mgy, Scan time: 11 seconds, MAS - 90, KV - 120; field of view - 180 mm. The scan revealed not only seven canals (three mesiobuccal, two palatal and two distobuccal) in left maxillary first molar (Figure 3A, 3B, 3C) but also existence of multiple canals in both maxillary first and second molars bilaterally (Figure 4A, 4B). At the second appointment, the patient was asymptomatic. After administering local anaesthesia 2% lignocaine containing 1:100,000 epinephrine (Xylocaine;Astrazeneca Pharma Ind Ltd,Bangalore,India) cleaning and shaping was done using crown down technique under rubber dam isolation with ProTaper nickel-titanium rotary instruments (Denstply Maillefer, Ballaigues, Switzerland).Irrigation was performed using normal saline,2.5% sodium hypochlorite solution, and 17%EDTA (ethylenediaminetetraacetic acid).The final irrigation was done with 2%chlorhexidine digluconate. The canals were dried with absorbent points(Denstply Maillefer, Ballaigues, Switzerland), master cone selection and the root canal space was obturated using cold lateral compaction of gutta percha (Denstply Maillefer, Ballaigues, Switzerland) with AH Plus resin sealer (Maillefer, Denstply, Konstanz, Germany) (Figure 5).The tooth was then restored with a posterior composite resin core(P60;3M Dental Products,St Paul,MN).After three months follow-up period , the patient was clinically asymptomatic and was advised a full-coverage porcelain crown.
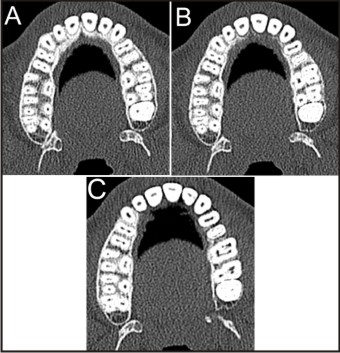 | Figure 3: SCT images of #26 showing axial sections at the (A) Apical 3rd, (B) Middle 3rd and (C) Coronal 3rd.
|
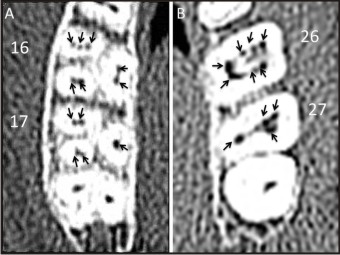 | Figure 4: Enlarged SCT axial images of #16, #17 and #26, #27 (arrows) showing multiple canal orifices respectively.
|
 | Figure 5: Post obturation radiograph(#26)
|
Discussion:
Cohen and Burns described the maxillary first molar as “...Possibly the most treated, least understood, posterior tooth”.[8] This case report emphasizes the methods of detecting additional canals using the latest adjuncts in successfully diagnosing and negotiating them which contribute to the successful outcome of root canal treatment. Endodontic access should be designed to provide direct access to apical third of root canal system, not merely to locate the canal orifice. Normally, MB3 canal is 0.5-5mm palatal to the main MB canal seen as discolored dot area. Therefore, full extent of the grooves on the floor of pulp chamber from mesiobuccal orifice to palatal orifice must be explored.[9] Hence, in this present case traditional triangular access opening was modified to trapezoidal shape.
The magnification plays another critically essential element giving the clinician unsurpassed vision, control, and confidence in identifying or chasing extra canals. With the help of conventional radiographs, complexity of canal system cannot be characterized due to the superimposition effects of the zygomatic bone.[10] Newer diagnostic methods such as computerized axial tomography (CT) and its applications in endodontics were first reported by Tachibana and Matsumoto in 1990. Spiral CT is a recent advance in CT technology. By using simultaneous patient translation through the X-ray source with continuous rotation of the source-detector assembly, SCT acquires raw production data with a spiral sampling locus during relatively short period viewed as conventional transaxial images such as multiplaner reconstructions or as 3-dimensional reconstructions, the possibility for missing dental structures is lessened.[11]CBCT scanning is a relatively newer diagnostic modality limited to major metropolitan areas, very expensive and include medicolegal issues.[4]
Methods of detecting additional canals :[5],[12]
1. Additional off- angle radiographs
2. Use of magnification (loupes and microscopes)
3. Examine the pulpal floor for “lines” to areas where additional canals can be located.
4. Ensure adequate “straight line “access to improve visibility.
5. Look for heamorrhagic spots.
6. Perform champagne test with sodium hypochlorite.
7. Staining the pulp chamber with 1%methylene blue.
8. Modify the conventional outline form to include extra canals.
9. White line test.
10. Removal of small amount of tooth structure that often may occlude a Canal Orifice (ultrasonic tips, round burs, tapering finishing burs)
In the present case, SCT confirmed the presence of three roots and seven canals, the following new nomenclature of additional canals MB1 (mesiobuccal / MB), MB2 (middle mesiobuccal / m-MB), MB3 (palato mesiobuccal / P-MB), DB1(distobuccal/ DB), DB2 (palatodistobuccal / P-DB)and MP( mesiopalatal), DP (Distopalatal).[12] The images showed that both distobuccal and palatal root presented Vertucci's type IV canal pattern(two canal orifices exit as two apical foramina),where as the mesiobuccal root had Vertucci's type VIII canal pattern (three canal orifices and exiting three foramina).[13] Another rare entity in this patient is the bilateral existence of multiple canals. The maxillary right first molar(#16) also showed seven canals ,the right second molar(#17) had five canals and the left second molar(#27) presented four canal orifices (Figure 4A, 4B ) .In doubtful cases where there is diagnostic dilemma about unusual canal systems; SCT is a good three dimensional investigative tool to confirm root canal morphology.
References
1. Malagnino V,Gallottini L,Passariello P. Some unusual clinical cases on root anatomy of permanent maxillary molars. J Endod 1997; 23:127-8.
2. Hess W, Zurcher E. The anatomy of the root canals of the teeth of the permanent and deciduous dentitions. New York: William Wood & Co., 1925.
3. Holderrieth S, Gernhardt CR. Maxillary molars with morphologic variations of thepalatal root canals: a report of four cases. J Endod 2009; 35:1060–5
4. Kottoor J, Velmurugan N,Sudha R, Hemamalathi S. Maxillary first molar with seven root canals diagnosed with cone beam computed tomography scanning:A case report.J Endod 2010; 36:915-21.
5. Karthikeyan K, Mahalaxmi S. New nomenclature for extra canals on four reported cases of maxillary first molars with six canals.J Endod 2010; 36:1073-8
6. Kottoor J, Hemalathi S, Sudha R, Velmurugan N. Maxillary second molar with 5 roots and 5 canals evaluated using cone beam computerized tomography: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010 feb; 109(2):e162-5.
7. Kottoor J, Velmurugan N, Surender S.Endodontic management of a maxillary first molar with eight root canal systems evaluated using cone-beam computed tomography scanning: a case report. J Endod. 2011 May; 37(5):715-9.
8. Burns RC. Access openings and tooth morphology. In: Cohens S, Burns RC, eds. Pathways of the pulp.4th ed. St.Louis: C.V.Mosby; 1987:120.
9. Johal S. Unusual maxillary first molar with 2 palatal canals within a single root:A case report. J Can Dent Assoc 2001; 67:211–4.
10. Slowey RR. Radiographic aids in the detection of extra root canals. Oral Surg Oral Med Oral Pathol 1974; 37:762-72.
11. Matherne RP, Christos A, Kulid JC, Tira D. Use of cone-beam computed tomography to identify root canal systems In Vitro.J Endod 2008; 34:87-9
12. Kottoor J, Albuquerque DV, Velmurugan N. A new anatomically based nomenclature for the roots androot Canals—Part 1: Maxillary molars.Int J Dent 2012; 2012:120565.
13. Vertucci FJ. Root canal morphology and its relationship to endodontic procedures. Endod Topics. 2005;10:3–29.
|