Introduction
Talon Cusp was first described as an anomalous hyperplasia of the cingulum of maxillary or mandibular permanent incisors resulting in the formation of a supernumerary cusp resembling an eagle's talon.[1],[2] However, there are reports of talon cusp occuring on the facial surfaces, in deciduoes incisors and also in canines. Therefore, the talon cusp can now be defined as an uncommon dental anamoly manifesting as an accessory cusp like structure, projecting from the lingual or facial surface of anterior teeth of either dentition.[3] It was first described by WH Mitchell in 1892 and was named as "Talon cusp" by Mellon and Ripa in 1970.[4]
The etiopathogenesis is multifactorial, and is thought to be polygenetic with some environmental influences.[5] Clinically it can pose esthetic and functional problems to the patient.[6],[7],[8],[9]. Histologically, it is composed of normal enamel & dentin & it may or may not contain pulpul tissue.[7] Radiographically the talon cusp is usually superimposed over the tooth on which it occurs. Hattab et al have classified talon cusp as true talon, semitalon and trace talon based on the degree of formation & extension. The treatment objective of talon cusp should include preserving pulpal vitality, meeting esthetic and occlusal requirement, establishing caries prevention or eradication in developmental grooves and eliminating tongue irritation.[7]
The objective of this article is to report a case of talon cusp in a permanent maxillary central incisor that required endodontic treatment.
Case Report
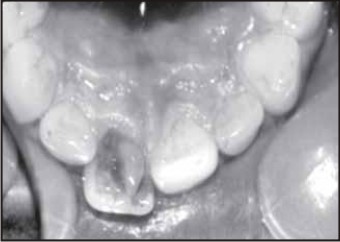
A 20 years old, male patient came to the department of oral surgery for extraction but considering restoribility of tooth, patient was referred to the department of conservative and endodontics. His medical & dental history was uneventful. No other family member had similar anamoly. Intra oral examination revealed no soft tissue abnormalities and absense of any tenderness to percussion. The tooth in question showed a concial prominent cusp on the palatal surface. The cusp was 2 mm wide (mesio distally), 6 mm (inciso cervically) and 3 mm thick (labiolingually) extending from cingulum area to the 0.5 mm short of incisal edge (Fig. 1) Electric and thermal pulp vitality tests showed tooth as a non vital entity. Radiographic examination showed the presence of enamel, dentin and pulp horn into talon cusp along with periradicular changes and rarefaction at periapical area (Fig. 2). The diagnosis was talon cusp with pulp necrosis. Single visit endodontic treatment was performed (Fig. 5) followed by intra and extra coronal bleaching using 35% H2O2
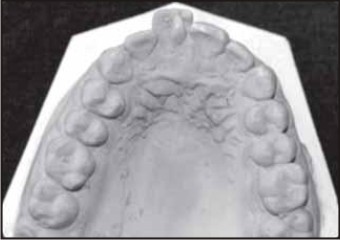 | Fig.1 : Preoperative Diagnostic Cast Depicting Talons Cusp
 |
 | Fig.2 : Pre –operative Radiograph
|
 | Fig.3 : Radiograph Showing Completed Endodontic Treatment
|
 | Fig.4 : Preoperative Palatal View
|
 | Fig.5 : Post Operative View
|
Discussion
Talon cusp or dens evaginatus is a rare anomaly with multifactorial etiology including both genetic and environmental factors. Various theories were proposed, however the most accepted one suggests that talon cusp might occur as a result of an outward folding of inner enamel epithelial cells and a transient focal hyperplasia of mesenchymal dental papilla. Hattab et al classified this anamoly into 3 types on the basis of the degree of cusp formation and extension. Type 1 (talon) has an additional cusp that projects from the palatal surface of an anterior tooth and extend at least one half the distance from the cemento enamel junction to the incisal edge. Type II (Semitalon) has an additional cusp 1 mm or more in length but extending less than one half the distance from the cement enamel junction to the incisal edge. Type III (trace talon) manifest enlarged and prominent cingula) and their variation. The talon cusp described in this case is classified as type 1 talon. It is important to remember that the talon cusp is occasionally combined with other systemic anamolies.
Clinically talon cusp differs from dens evaginatus of posterior teeth. Lin et al reported pulp exposure and pulp necrosis in 14.1% to 40.2% of examined cases due to attrition or trauma. Developmental grooves and fissures at the junction of the talon cusp and the tooth surfaces are more susceptible to caries, depending on the shape, size and location of these structural defects, associated periodontal involvement might occur.
Gungor et al histologically detected presence of pulp horn in accessory cusp which increases the chances of pulpal insult & death. Teeth with talon cusp may undergo pulpal necrosis if early diagnosis is not done & management is neglected or inappropriate to the case.
The treatment of talon cusp may be conservative or radical, depending on the accessory cusp like shape, location, size & tooth affected. Periodic & gradual reduction of the cusp, with application of the desensitizing agent, reduction of cusp with or without endodontic therapy, sealant application on the grooves and esthetic restorations are options of treatment. Single visit root canal offers several advantages likewise reduced flare rate (Walton & Faud 1992), patient acceptance and practice management. 70% of dentists treat necrotic teeth in single visit since it has shown 6.3% higher healing rate than multiple visit.[9] Bleaching can improve the appearance of discoloured teeth while preserving tooth structure and it avoids costly invasive dental tratment. Cadanaro M et al showed in vivo application of 38% H2O2 and 35% carbamide peroxide to be clinically safe & reliable, showing no structural changes to enamel surface even after four applications.[10] The treatment objective for taloned teeth may differ depending on each case. However large, prominent talon cusp calls for a definitive treatment to overcome esthetic, occlusal, periodontal & carious problem.
Conclusion
Talon cusp is not an innocuous defect, as it may provide a substantial challenge during diagnosis and treatment planning to clinician. Early diagnosis may minimize local problems such as caries, periodontal disease & carious problems.
References
1. Shafer W G, Hine MK, Levy BM. A textbook of oral pathology. 4th ed, Philadelphia : WB Saunders 1983, 40-41
2. Goaz PW, White SC Oral Radiology, Missouri : CV Mosby company; 1987;447
3. Sirace E, Cem Gugnor H, Taner B, Cehrili ZC. Buccal & palatal talon cusps with pulp extensions on a supernumerary primary tooth. Dentomaxillofacial Radiology 2006 : 35(6) : 469-72
4. Mellor JK, Ripa LW, Talon cusp : A clinically significant anamoly. Oral surg 1970 ; 29 : 225-28
5. Segura JJ, Jemenez, Rubro A-Talon cusp affecting permanent maxillary lateral incisiors in 2 family members Oral surg Oral Med Oral Pathol Oral Radiol Endod 1999 ; 88 (1) : 90-92
6. Hattab FN, Yassin OM, al Nimri KS. Talon cuspin permanent dentition associated with other dental anamolies : Review of literature and reports of seven cases ASDCJ Dent child 1996;63(5) : 368-76
7. H. Cm Gungor, Nil Altay & Figen Kaymaz, Ankara. Pulpal issue in bilateral talon cusps of primary central incisor. Report of a case. Oral Surg Oral Med Pathol Oral Radiol Endol 2000; 89:231-5
8. Andeesa Bolges Soares et al. Bilateral talon cusp : Case Report. Quintessence Int 2001;32-283-286
9. Salhorn C, Messer HH, Effectiveness of single wersus multiple visit endodontic treatment of teeth with apical periodontitis : a systemic review and meta analysis. Int Endod J 2005 ; 38 : 347-355
10. Cadenaro M et al, Effect of two in-office whitening agents on the enamel surface in vivo : a morphological and non contact profilometric study. Operative dentistry 2008, 33-2:127-134.
|