Introduction
The separation of instruments during endodontic therapy is a troublesome incident, and its incidence ranges from 2% to 6% of the cases investigated.[1] Successful endodontic treatment depends on a series of sequential procedures including cleaning and shaping of the root canal system. Procedural errors such as ledging, zipping, canal perforation and apex transportation can occur during root canal instrumentation. However, separation of endodontic instruments (SEF) is a problematic incident. Conflicting results have been reported regarding the clinical significance of fractured files remaining within treated root canals.[1] Therefore, when an instrument fractures in the root canal, the clinician must evaluate carefully the options of attempting to remove the instrument, attempting to bypass the instrument, or preparing and filling to the fractured instrument (Suter et al. 2005).[2]
Many techniques, methods and instruments have been proposed for the removal of foreign bodies, broken instruments, silver cones and cemented posts in root canals, i.e., Canal Finder system, Masseran Kit, Endo Extractor System, Ultrasonics, and several kinds of pliers. Feldman et al. (1974) reported the removal of broken instruments from single root and multiple roots with the Endo Extractor System. Sieraski and Zillich (1993) used the ultrasonic scaler that produces less dentin wear as already reported by Souyave et al. (1985) and Meidinger and Kabes (1985). The Canal Finder System can also be used successfully according to Hüllsman (1990) in an experimental and clinical study.
Fors and Berg (1993) reported a clinical case of removal of a broken file in the mesio-buccal canal of a mandibular third molar using a micro-surgical Castroviejos needle holder for ophthalmology. Weissman (1993) also reported the use of a perry pliers for removal of a silver cone.
Many guidelines have been suggested for the prevention of SEF. Most are related to the operator, including:
• Instrument should be examined ,before and after use,to make certain that blades are regular aligned
• Instrument should not be used in dry canals
• Files should be used according to the manufacturer’s instruction and excessive forces should be avoided.
There is a variety of protocol for root canal instrument. Experience of file separation was found to differ not only beween different dental practitioners, but also at different times for the same practitioners.[3],[4]
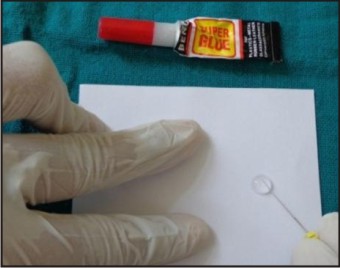
Varying extents of tooth structure are removed during this procedure which may potentially cause complications. There is no doubt that the degree of curvature is one of most important factors influencing the successful management of separated instruments[5]. However, fragments present in the root canal can hinder proper preparation of root canal space. A technique as devised by rowe uses cyanoacrylate glue {permabond or super glue # 30 } and hypodermic needle to retrieve silver point. According to it when a silver point is not protruding into the pulp chamber then select a hypodermic needle that fits snugly over silver point remove the bevel of needle and cement it over the silver point using cyanocarylate glue after 5 minutes of setting time the needle is grasped the hemostat and silver point worried from place. [6]
Following case describes the clinical scenario of fractured fragment removal by the use of cyanocarylate glue
Case Report
This clinical endodontic study was performed in an endodontic department in Mullana, Ambala.
A 38 year old male patient reported with the history of pain in lower right back teeth since one month. On examination, there was a deep dental caries on the lower right first molar. On radiographic examination radiolucency was seen in dentin on the mesial buccal encroaching the pulp space. Root canal treatment was decided as the treatment for the tooth.
Clinical sequence
The clinical procedure consists of consecutive steps:
The aim is to achieve direct access to the fragment while removing as little dentin as possible. Instrument fractures in the coronal or middle third of the root canal are most frequently caused by incorrect preparation of the access cavity or the presence of a curve in the coronal third of the canal. The first step is, therefore, dedicated to rectifying the canal access and relocating the coronal entrance. This requires straightening of the canal wall opposite the curve.[7],[8]
• A cylindro-conical bur with non-cutting tip for straightening
• the walls of the access cavity
• A short Gates Glidden size 4 for relocation of the canal entrance, which is moved along the wall opposite the coronal curve with vertical back-and-forth movements
• A Gates Glidden size 3 to prepare access to the fragment
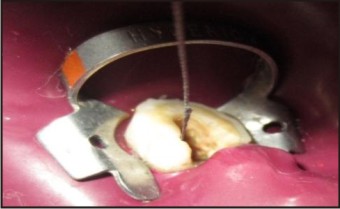
Local anaesthesia was administered (Xylocaine 2% adrenaline). Isolation was done using rubber dam (Hygenic, Coltene/Whaledent Inc). Access opening was done using endo-access bur. Initial exploration of the canal was done using K file #10. K file #15 was the next instrument used in the canal. K file #15 instrument fracture was observed in the distobuccal canal of the tooth. A radiograph was taken to confirm the instrument separation. In the radiograph, the instrument was seen extending from the apical third to the coronal orifice of the canal (Figure 1).
Gates glidden drill was also used for the enlarging root canal. Appropriately sized ULTRASONIC instrument was selected, such that the length will reached to the broken obstruction and its diameter will passively fit into the previously shaped canal. Then the ultrasonic instrument was placed in intimate contact against the obstruction and typically then it was activated within the lower power setting.
Ultrasonic action trephines, sands away the dentin and exposes the coronal few millimeters of the obstruction begins to loosen, unwind and then spin. And it was revealed that the instrument could be partially bypassed and that it was loose within the root canal.
After Drying The Canal with 20 no k file was taken and the cyanoacrlate adhesive was applied onto the file (Figure2). then taken into the canal that will adhere firmly with the broken instrument (Figure3). and after not moving the combination slowly in coronal direction Will Bring The Broken Instrument Safely Out Of The Canal. (Figure 4, 5). When instrument removal was completed and before obturation, a radiograph was taken to confirm whether the instrument was absent as in successful cases or in the case of failure, the size and location of the remaining fragment. Success was defined as complete removal of the fractured instrument from the root canal without creating a perforation (Figure 6). The canal was then routinely prepared and all canals filled with lateral compaction of gutta-percha and AH26 (Dentsply) sealer (Fig. 7).
 | Figure 1
 |
 | Figure 2
|
 | Figure 3
|
 | Figure 4
|
 | Figure 5
|
 | Figure 6
|
 | Figure 7
|
Discussion
Morphological variations in root canal system anatomy should always be considered at the beginning of treatment. Each case, independently of the type of tooth, should be examined carefully, clinically and radiographically in order to detect possible anatomical aberrations.[9] Intracanal separation of instruments usually prevents access to the apex, impedes thorough cleaning and shaping of the root canal, and thus may compromise the outcome of endodontic treatment and reduce the chances of successful retreatment. In such cases, prognosis following an endodontic therapy depends on the condition of the root canal (vital or nonvital), tooth (symptomatic or asymptomatic, with or without periapical pathology), level of cleaning and shaping at the time of separation, the level of separation in the canal; and is generally lower than that with normal endodontic treatment.[10]
Factors should be considered when treatment planning fractured instrument case :
• Preoperative pulpal and periapical diagnosis
• Extent of chemo-mechanical debridement prior to instrument breakage
• Position of fractured instrument, i.e. direct vision and adequate straight line access ?
• Length of fragment
• Anatomy of the root (thickness, presence of concavities and curvature of the root canal)
• Can the instrument be bypassed? If yes, bypass it and do not actively attempt removal. [11]
clinical practices in endodontics that the use of magnification is considered helpful for the successful completion of endodontic treatment. According to endodontic literature, the MM canal can be found in 1–15% of the cases .
In most of the cases, this canal is hidden by a dentinal projection of the mesial aspect of pulp chamber walls. In all cases of mandibular molars, this dentinal growth is usually located between the two main canals and should be removed carefully in order to detect the additional canal or canals. Ultrasound technology is a very useful tool for the clinician to clean such an area efficiently.
Removal of the fractured instruments is more influenced by the anatomy of tooth, degree of root canal curvature and the location of the fragment than the specific technique used. Success rate can be quite variable because removal of the fractured instruments is difficult and time-consuming. A technique utilising modified Gates–Glidden burs and ultrasonic has recently been advocated to remove fractured instruments from root canals. Varying extents of tooth structure are removed during this procedure which may potentially cause complications. There is no doubt that the degree of curvature is one of most important factors influencing the successful management of separated instruments [12].
A technique as devised by rowe uses cyanoacrylate glue {permabond or super glue # 30 } and hypodermic needle to retrieve silver point. According to it when a silver point is not protruding into the pulp chamber then select a hypodermic needle that fits snugly over silver point remove the bevel of needle and cement it over the silver point using cyanocarylate glue after 5 minutes of setting time the needle is grasped the hemostat and silver point worried from place.[13]
Although the short term sealability success of silver point seemed comparable to that of gutta perch, silver point are a poor long term choice as routine obturation materal.[14]
Factors Influencing Broken Instrument Removal
Success of retrieval depends on the canal anatomy, what type of metal the piece is made out of (stainless steel files tend to be easier to remove), the location in the canal of the fragment, the plane in which the canal curves, the length of the separated fragment, and the diameter of the canal itself[15]. In general, if one third of the overall length of an obstruction can be exposed, it can usually be removed.
Instruments that lie in the straightaway portions of a canal can typically be removed. More challenging are separated instruments that lie partially around canal curvatures, but these can often be removed if straight-line access can be established to their most coronal extents. If the broken instrument segment is apical to the curvature of the canal and safe access cannot be accomplished, then removal is usually not possible.
Conclusion
Conventional Techniques Must Be Tried But If They Prove To Be Unsuccessful, Alternative Method - Cyanoacrylate Glue Helped For Removal Of Broken Endodontic Instruments.
Method Is Simple, Cost Effective And At The Same Time Can Result In Predictable Success
The best antidote for a broken file is prevention. Adhering to proven concepts, integrating best strategies and utilizing safe techniques during root canal preparation procedures will virtually eliminate the broken instrument procedural accident.[16],[17],[18]
References
1. Arcangelo CM, Varvara G, Fazio PD. Broken instrument removal two cases. J Endod. 2000;26:568–70.
2. A. Madarati,1 D. C. Watts2 and A. J. E. Qualtro. Factors contributing to the separation of endodontic files. British Dental Journal Volume 204 NO. 5 MAR 8 2008.
3. Ruddle CJ: Ch. 8, Cleaning and shaping root canal systems. In Cohen S, Burns RC, editors: Pathways of the Pulp, 8th ed., Mosby, St. Louis, pp. 231-291, 2001.
4. Shikha gulati. Retreatrment of silver point obturation A case report and an overview.journal of contemporary dentistry. Sep- Dec 2012,2(3):114-118.
5. M. Rahimi & P. Parashos A novel technique for the removal of fractured instruments in the apical third curved root canals. International Endodontic Journal, 42, 264–270, 2009.
6. Shen Y, Peng B, Cheung GS. Factors associated with the removal of fractured NiTi instruments from root canal systems. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2004; 98: 605–10.
7. Ruddle CJ.: Broken Instrument Removal: The Endodontic Challenge, Dentistry Today, July 2002.
8. Mandel E, Adib-Yazdi M, Benhamou LM, Lachkar T. Rotary Ni-Ti profile systems forpreparing curved canals in resin blocks: influence of operator on instrument breakage. Int Endo J 1999;32: 436-443.
9. Shikha gulati. Retreatrment of silver point obturation A case report and an overview.journal of contemporary dentistry. Sep- Dec 2012,2(3):114-118. Farhad Faramarzi, DDS, MSD1; Hamidreza Fakri, DDS2; Homan H Javaheri, DDS2..
10. Farhad Faramarzi, DDS, MSD1; Hamidreza Fakri, DDS2; Homan H Javaheri, DDS2. Endodontic treatment of a mandibular first molar with three mesial canals and broken instrument removal.Aust Endod J 2010; 36: 39–41
11. Arun Kulandaivelu Thirumalai, Mahalaxmi Sekar, and Sumitha Mylswamy. Retrieval of a separated instrument using Masserann technique J Conserv Dent. 2008 Jan-Mar; 11(1): 42–45.
12. Peter Parashos, MDSc, PhDemail, Harold H. Messer, MDSc, PhD Journal of Endodontics 32, 1031–43.2006Rotary NiTi Instrument Fracture and its Consequences.
13. Shen Y, Peng B, Cheung GS. Factors associated with the removal of fractured NiTi instruments from root canal systems. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2004; 98: 605–10.
14. Studio 2050, producer: Ruddle on clean shape pack, 2-tape video series, Advanced Endodontics, Santa Barbara, 2002.
15. Marnding M, Lutz F,Barbakow F. Scanning electron microscope appearances of lightspeed instruments used clinically : a pilot study. Int Endod J 1998; 31:57-62.
16. Yared Gm, Dagher F E, Machtou P,Kulkarni G K. Influence of rotational speed, torque, and operator proficiency on failure of greater taper files. Int Endod J 2002,35: 7-12.
17. Parashos P,Gordon I, Messer H H. Factors influencing defect of rotary nickel-titanium endodontic instruments after clinical use. J Endo 2004;30:722-725
18. Iqbal M K, Kohli M R , Kim J S. A retrospective clinical study of incidence of root canal instrument separation in an endodonticsgraduate program: a pennEndodata base study. J Endo 2006;32:1048-1052.
|