Introduction
Dental plaque is regarded as the main etiologic factor of periodontal disease. The role of dental plaque in the development of plaque-induced gingivitis and chronic periodontitis is well established[14],[21],[23],[27]. It is believed that the best approach to manage periodontal disease is prevention followed by early detection and treatment. The prevention of periodontal disease is targeted at the control of dental plaque. Both mechanical and chemicomechanical concepts have been developed to reduce or prevent the development of periodontal diseases.[8],[17]
Oral health is related to diet in many ways, associations have been suggested between nutritional in@258;uences and craniofacial development, oral cancer and oral infectious diseases[1]. The consumption of fibrous food has been positively correlated with the prevention of periodontal diseases by reducing the amount of dental plaque[8],[11]. Of these hard foods, apples have been the most commonly recommended. Apples have commonly featured in dental health programmes and have become, to some extent, a symbol of dental health.[8],[11],[22],[23]
While many studies correlating the effect of fibrous food on plaque deposits on teeth are available[8],[11],[22],[23], the authors could not find any data on plaque controlling effect of fibrous food at different sites of teeth. This study was therefore designed to study the relative additional mechanical plaque controlling/removing effect of fibrous food (apple) as a plaque controlling agent at different sites (i.e. different selected teeth and different zones on the labial surface of these selected teeth) over and above the routine tooth brushing and/or other physical and chemical plaque control measures already being practiced by the individual.
Materials And Methods
Materials
Fibrous food (Apple), Two tone plaque disclosing solution (Dye ‘Alpha Plac’ Dental products of India, The Bombay Burmah trading corporation ltd.), Mouth mirror, Cheek retractor, Tweezers, Cotton rolls.
Method
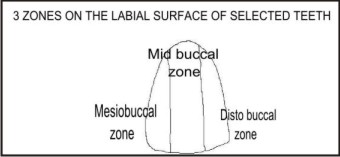
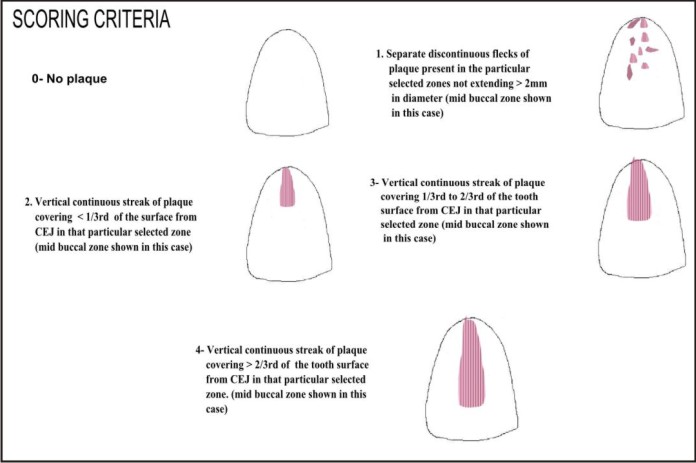
A total of 100 healthy subjects which included 4th year students and interns of Baba Jaswant Singh Dental College and hospital, Ludhiana, were selected for the study. A written informed consent was taken from all the subjects participating in the study. In all the cases teeth number: 11, 15, 25, 35, 41 & 45 (FDI notation) were selected for assessment of plaque. Labial surface of the selected teeth was divided into three virtual vertical zones i.e. mesiobuccal 1/3rd, mid buccal 1/3rd and distobuccal 1/3rd for assessment of plaque deposits (Diagram 1). All the subjects were asked to continue any and all plaque control measures (physical and/or chemical) already being practiced by them. Within one hour of toothbrushing, an apple of almost equal size and weight was distributed to each student and the plaque scoring was done for each student before (Prescore) and after they ate an apple after staining the teeth(Post score) using ‘Alpha Plac’ two tone disclosing dye solution. The extent of plaque on the selected surfaces of each tooth was calibrated using the following criteria (Diagram 2). Score 0 was for no plaque on the selected particular tooth surface. Score 1 was assigned to separate discontinuous flecks of plaque not exceeding 2mm in diameter in that particular selected zones. Score 2 was assigned to vertical streaks of plaque covering < 1/3rd of the tooth surface from CEJ in that particular selected zone. Score 3 was assigned to vertical streaks of plaque covering 1/3rd to 2/3rd of the tooth surface from CEJ in that particular selected zone. Score 4 was assigned to vertical streaks of plaque covering > 2/3rdof the tooth surface from CEJ in that particular selected zone (Diagram 2).
 | Diagram 1
 |
 | Diagram 2
|
Results
The data thus collected was tabulated (Table 1,2,3 and 4) and put to statistical analysis. Paired t test was used to compare the change in the total mean plaque scores in all the teeth. For comparing the change in plaque between different teeth and also between 3 different tooth surfaces ANOVA was used.
As is evident from the data collected, the results of the above study show that ongoing plaque control methods practiced by the subjects were not completely effective in removing all the plaque from the selected teeth (as the plaque deposits were seen on all selected tooth surfaces/zones). The mean plaque pre score of all the three surfaces in the 6 selected teeth of the 100 cases was 2.17 and the mean plaque post score value after chewing the apple was 1.06 with a highly significant difference of 1.11 (Table1) [it must be mentioned here that some sites did not show any / remarkable change i.e., reduction in post plaque scores].
The distobuccal zones of all the selected teeth showed the maximum remaining plaque [pre score] inspite of regular plaque control measures being practiced by the individual selected for the study, followed by the mesiobuccal zones and the midbuccal zones (Table3).
 | Table 1. Change In Plaque Scores In All The Evaluated Teeth.
|
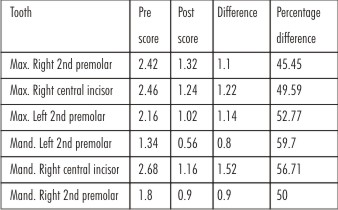 | Table 2. Change In Plaque Scores In Individual Teeth.
|
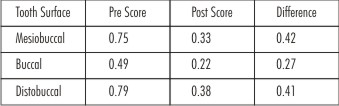 | Table 3. Change In Mean Plaque Scores On The Three Intra-tooth Vertical Zones
|
![Table 4. Percentage Changes In The Pre-scores [Pre Fibrous Food] And Post-scores [Post Fibrous Food] On The Three Surfaces Of Evaluated Teeth.](article-image-4652-TABLE_4._PERCENTAGE_CHANGES_IN_THE_PRE_SCORES_[PRE.jpg) | Table 4. Percentage Changes In The Pre-scores [Pre Fibrous Food] And Post-scores [Post Fibrous Food] On The Three Surfaces Of Evaluated Teeth.
|
Of all the selected zones, distobuccal zone of the tooth no.41 showed the maximum prescore plaque deposit (0.96) and the midbuccal zone of tooth no. 45 showed the minimum prescore plaque deposit (0.18) (Table4). Comparison in the changes in plaque among the three vertical zones showed maximum reduction on the mesiobuccal surface (0.42) and the minimum on the midbuccal surface (0.27) in all the selected tooth surfaces/zones (Table 3).
Out of all the selected teeth the mid buccal zone of tooth no.41 showed the maximum percentage change (71.8%) and distobuccal zone of tooth no.11 showed the minimum percentage change (43.2%) in the plaque scores after consumption of fibrous food, although the total [all three zones combined] inter tooth difference in plaque score was non- significant (Table 4).
Discussion
It is proved beyond doubt that the presence of dental plaque is absolutely essential for development of periodontal diseases[14]. The bacterial plaque initiates inflammatory process in the supporting structures of the tooth and if allowed to continue, will ultimately lead to the loss of teeth. For this reason intra-oral cleansing devices have been a part of the human civilization since ages. Mechanical supragingival plaque control is the most rational and efficient method for the prevention of periodontal diseases.[9] Daily removal of plaque by the patient is also of concern for a beneficial long-term treatment outcome. The effective use of mechanical devices to reduce dental plaque, in fact, is highly dependent on patient compliance with oral hygiene instructions given by dental professionals. A majority of individuals find it difficult or even impossible to comply with a proper oral hygiene regimen. Moreover, even in those patients who do achieve high levels of oral cleanliness after instructions, plaque control deteriorates over time.[16],[17] Reasons for non-compliance are many and may include level of education, domestic circumstances, disposable income, beliefs and attitudes regarding personal and oral care, stressful life events, psychomotor skills, frequency of dental visit, and age.[18],[20] Thus, adjunctive methods of mechanical plaque removal are essential and beneficial.
Fibrous food eating fits in here and it has been encouraged in the past due to many reasons. It is an age old belief that apple eating after meals cleaned the teeth[8],[11] and it removed food residues and plaque[22],[23]. This favourable effect of chewing apples though is seen across all age groups, but may not be same in all individuals and all areas of oral cavity.
The present study was therefore conducted with an objective of assessing the additional plaque removing effect of fibrous food (apples) on different teeth and different individual zones on labial teeth surfaces. Results of this study show that the mean plaque prescore of all the three selected surfaces in the 6 selected teeth of 100 subjects was 2.17 and the mean plaque post score value after chewing the apple was 1.06. There is a highly significant difference in the prescore and post score plaque levels [1.11]. When the comparison was made between the 6 selected teeth for the change in plaque scores, maximum percentage reductions were seen in tooth no.35 and minimum in tooth no.15, although the intertooth difference in plaque score reduction was non-significant when all sites on six teeth were evaluated together. On comparing the changes in plaque score among the 3 vertical zones of all selected teeth, maximum reduction in plaque scores was seen on the mesiobuccal surface (0.42) and minimum on the midbuccal surface (0.27). When changes in the individual teeth surfaces were analysed, it was observed that distobuccal zone and mesiobuccal zone of the tooth no. 41 had the highest deposit of plaque even after ongoing and already being practiced plaque control measures and the distobuccal and the midbuccal zone of tooth no.35 had the minimum. These results show that the regular plaque control measures practiced by the individual are not sufficient to achieve the desired reduction in plaque deposit. These results are in accordance with the epidemiological studies in the past which have shown clearly that there are certain key-risk-teeth (molars and premolars) and key risk- surfaces (the proximal surfaces of the molars and premolars).[3]
In our study after the consumption of apple, the midbuccal zone and mesiobuccal zone of tooth no. 41 showed the maximum percentage change (reductions) in plaque score and the midbuccal zone and distobuccal zone of tooth no. 15 showed the minimum percentage reduction in plaque scores.
Although it was found that some teeth surfaces did not show any change (reduction) in the pre and post plaque scores after consumption of fibrous food but when analysed as a whole, the above observations suggest a considerable cleansing action of fibrous foods (apples) on the supragingival plaque. It can also be inferred that of all the teeth lower anteriors are less amenable to plaque control/removal by routinely practiced oral hygiene measures alone as they showed highest plaque pre plaque scores. The lower anterior teeth also showed the maximum percentage reduction in plaque scores after chewing fibrous food. (Table4, Graph2). Greater reductions in plaque scores in the mandibular anterior teeth may be related to the more relative usage of these teeth as compared to maxillary teeth especially during initial biting of apples. The greater reduction on the mesiobuccal and distobuccal zones as compared to midbuccal zone can be related to the presence of embrasures adjacent to these zones. These embrasures probably make tooth brushing more cumbersome but allow comparatively greater effective cleansing of the adjacent tooth zones when the fibrous food being masticated rubs past them through these embrasures. This is also clear from the results where the distobuccal and mesiobuccal zones show higher plaque prescores in general than the midbuccal zones.
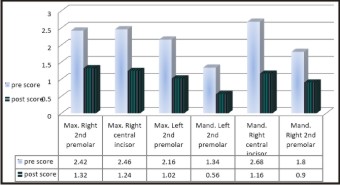 | Graph 1. Changes (Reductions) In Plaque Score In The Six Selected Teeth After Eating Fibrous Food (Apple)
|
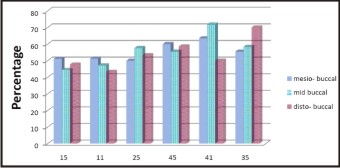 | Graph 2. Percentage Changes (Reductions) In The Pre-fibrous And Post-fibrous Scores On The Three Surfaces Of Evaluated Teeth.
|
Conclusion
There is a strong correlation between brushing frequency and the reduction in plaque/gingivitis on the buccal surfaces. The vast majority of self-taught toothbrushers begin by scrubbing the buccal surfaces, especially at the frontal region, and rarely proceed to the lingual surfaces. Interproximal cleaning is simply non-existent in the self-taught. The basic principle for preventive dentistry is that the preventive measures will give the most significant effect if we concentrate them on "key-risk age groups," "key-risk individuals," "key-risk teeth" and "key-risk surfaces." Thus there is a need of suggesting and incorporating adjunctive plaque control measures in the patient’s oral hygiene regimen. The following conclusion can be drawn from this study: routinely practiced oral cleansing/plaque control is not 100% effective. The mandibular incisors are the least amenable to cleansing by tooth brushing whereas the mandibular premolars are most amenable to cleansing by tooth brushing. Fibrous food helps to reduce the plaque scores in all the teeth. Chewing of apples causes a significant reduction in supra-gingival plaque levels. The mandibular teeth are more amenable to tooth cleansing by the use of fibrous food than the maxillary teeth particularly the midbuccal zone of mandibular incisors and distobuccal zone of premolars, whereas the maxillary premolars are the least affected teeth in relation to the cleansing action by the use of fibrous foods. The results of the study encourage the use of the fibrous foods in the diet due to their favourable effects on the gingival health. Within the limits of the study it may be safe to suggest that as plaque control is relatively more difficult at various sites i.e., distobuccal and mesiobuccal zones. These sites must be carefully monitored by the dental surgeons during maintenance visits as they may be the first sites where periodontal disease might show up again. Patients must also be educated and cautioned about maintaining good oral hygiene at these sites.
References
1. Anderson J and Barbara Deskins MS. "The Nutrition Bible"; RD; 1997
2. Axelsson P, Nystrom B, Lindhe J. The long term effect of a plaque control program on tooth mortality, caries and periodontal disease in adults. Results after 30 years of maintenance. Journal of Clinical Periodontology. 2003;30 (Suppl 5):4–6.
3. Axelsson P.: The effect of plaque control procedures on gingivitis, periodontitis and dental caries, Thesis, 1978.
4. Birkeland J.M. & Jorkjend L: the effect of chewing apples on dental plaque and food debris. Community dent. Oral Epidemiol.1974:2:161-162.
5. Bjorn, A. L.: Dental health in relation to age and dental care, Odont Re,z, 25: suppl. 29, 1974.
6. Ciancio S. Improving oral health: Current considerations. J Clin Periodontol. 2003;30 (Suppl 5):4–6.
7. Garmyn P, van Steennberghe D, Quirynen M. Efficacy of plaque control in the maintenance of gingival health: Plaque control in primary and secondary prevention. In: Lang NP, Attstrom R, Loe H, editors. Proceedings of the European workshop on mechanical plaque control. Berlin: Quintessenz Verla; 1998. pp. 107–20.
8. Knighton H.T. : effect of various foods and cleansing agents on the elimination of artificially inoculated yeast from the mouth. Journal of American dental association. 1942:29:2012-2018.
9. Lang, N. P., Cumming, B. R. and Lee H.: Tooth brushing frequency as it relates to plaque development and gingival health, J Periodontal, 7:396, 1973.
10. Lance L.S.: oral carbohydrate clearance.: nutrition and caries prevention. Almquist & Wiksell, Upsala 1965:53-59.
11. Lindhe, J &Wicen, PO.: The effects on the gingivae of chewing fibrous foods. J. Periodontal Res. 1969: 4: 193-201.
12. Lindhe, J., Hamp, S. E. and Loe, H.: Plaque-induced periodontal disease in beagle dogs, JPeriodont Rex, 10:243, 1975.
13. Listgarten, M. A.: Structure of the microbial flora associated with periodontal health and disease in man, J Periodont, 47:1,1976.
14. Loe H., Theilade E. &Jensen SB.: Experimental gingivitis in man. J. Periodontol. 1965: 36: 177-187.
15. periodontal disease and caries, Oral Sciences Rev, 9:23, 1976.
16. Renvert S, Glavind L. Individualized instruction and compliance in oral hygiene practices: Recommendations and means of delivery. In: Lang NP, Attstrom R, Loe H, editors. Proceedings of the European workshop on mechanical plaque contro. Berlin: Quintessenz Verlag; 1998. pp. 300–309.
17. Sangnes, G., Zaghrisson, B. &Gjermo, P.: Effectiveness of vertical and horizontal brushing techniques in plaque removal. J. Dent. Child. 1972: 39: 94-97.
18. Sanz M, Herrera D. Role of oral hygiene during the healing phase of periodontal therapy. In: Lang NP, Attstrom R, Loe H, editors. Proceedings of the European workshop on mechanical plaque control.Berlin: Quintessenz Verlag; 1998. pp. 248–67.
19. Saxe, S. R., Greene, J. C., Bohannan, H. M. and Vermilion, J. R.: Oral debris, calculus and periodontal disease in the beagle dog, Periodontics, 5:217, 1967.
20. Schou L. Behavioral aspects of dental plaque control measures: An oral health promotion perspective. In: Lang NP, Attstrom R, Loe H, editors. Proceedings of the European workshop on mechanical plaque control. Berlin: Quintessenz Verlag; 1998. pp. 287–99.
21. Silness, J. &LoE, H.: Periodontal disease in pregnancy. II. Correlation between oral hygiene and periodontal condition. AetaOdontol. Scand. 1964: 22:121-135.
22. Slack, G. L. &Martin, W. J.: Apples and dental health. Br. Dent. J. 1958: 105: 366-371
23. Socransky SS and Haffajee AD. The Bacterial Etiology of Destructive Periodontal Disease: Current Concepts. Journal of Periodontology1992;63:332-331
24. Theilade, E. and Theilade, J.: Role of plaque in the etiology of
25. van der Weijden GA, Hioe KP. Asystematic review of the effectiveness of self performed mechanical plaque removal in adults with gingivitis using a manual toothbrush. J Clin Periodontol. 2005;32(Suppl 6):214–228.
26. Wade, A. B.: Effect on dental plaque of chewing apples. Dent. Praet. Dent. Rec. 1971: 21: 1974-196.
27. Wallace, J S, The Physiology of Oral Hygiene and Recent Research, 2nd edn.
28. Zaki, H. A. and Bandt, C. L.: The effective use of a self-teaching oral hygiene manual, Journal of Periodontology 1974.45:491
|