Introduction
Traumatic dental injuries are the most unanticipated events frequently associated with childhood. The incidence of these injuries has markedly increased during the last 10 to 20 years, which suggests its incidence will soon exceed dental caries and periodontal diseases due to high level of violence, road traffic accidents and greater participation in sports[1].
These injuries not only compromise dental health, but can also lead to aesthetic, psychological, social and therapeutic problems. Hamilton et al[2] and Burton et al[3] stated that 6-34% individuals respectively suffer from traumatic dental injuries during their life. The 7- 12 year age group is considered to be most prone to any form of dental trauma because children of this age are engaged in lots of outdoor activities. According to the earlier literature, boys sustained dental trauma almost twice as much as girls, exhibiting significant gender difference with regard to dental trauma experience[1], [4]. According to Nik-Hussein[5], males experienced 5.5% trauma whereas females experienced only 2.8%. But recent studies have shown a reduction in this gender difference because of increased outdoor activities by girls[6],[7],[8].
Since most of the dental injuries can be prevented, so understanding the factors that predispose to trauma is essential for developing a concept for the prevention. Although, there are a number of studies that have determined the incidence and prevalence of dental trauma in various parts of India, but lack of such data has been found in the hills of Himachal Pradesh, which has a different geographical terrain. Hence the study was undertaken with the aim and objective of determining the prevalence of dental trauma and its correlating factors in District Mandi, Himachal Pradesh. This study gives a more detailed insight into the context and factors associated with the traumatic dental injuries in the children of Himachal Pradesh.
Material and method
Selection of Sample
A cross sectional study was carried out on a total of 1130 school going children between the age range of 8 to 12 years who were permanent residents of District Mandi, Himachal Pradesh. The children were further categorized into 8 yrs, 9yrs, 10yrs, 11yrs and 12yrs age groups among boys and girls respectively.The study was conducted in 6 randomly selected schools of the area, enrolling approximately 300 students per school with roughly equal number of boys and girls. Formal approval was taken from the principal. Ethical clearance was obtained by the ethical committee of the institute.
Inclusion criteria
-Children willing to participate with consent from duly signed by the parents or guardians.
Exclusion criteria
-Uncooperative children
-Medically compromised children.
-Children showing clinical evidence of trauma but without any relevant history, as the study was based on self-report of children.
Equipment-Mouth mirrors, tweezers, periodontal probes, disposable tongue depressors and cotton gauge pieces
Clinical Examination
Before examination the teeth were cleaned. Clinical examination was carried out in the school under natural day light. The examination was carried out by trained examiner and assistant. While examining the patient, the trained assistant was made to sit close to the patient, to record the data on specially designed proforma.
Examination was performed in a uniform fashion starting from the maxillary right quadrant to the mandibular right quadrant in a clockwise direction. The examination consisted of recording of age, gender, type of injury, cause of injury and place of injury. Injuries to the permanent teeth were categorized according to Ellis and Davey’s classification (1960) of tooth fracture. Only three criteria’s were included to classify the tooth fractures they were fracture of enamel/ enamel chipping (Ellis class I tooth fracture), fracture of enamel with involvement of dentine (Ellis class II tooth fracture) & fracture of enamel involving dentine and pulp (Ellis class III tooth fracture).
Repeated sessions of calibrations were performed by examiner and a supervisor to standardize recording procedure. Chronological age was the criteria for deciding the age of the patient.The data obtained was subsequently processed and analyzed using SPSS statistical software Program. The Chi-square test was employed to evaluate the results. The P-value < 0.05 was considered as statistically significant.
Results
In the present study,out of the 1130 children (571 males and 559 females), males showed higher percentage of TDI than females i.e (29.4%) as compared to (28.4%) (Figure1). Males had greater prevalence of trauma in 9 years (13%) while females had greater trauma in 10years (12.9%) age group and the difference was statically significant (p<0.05) (Table 1).
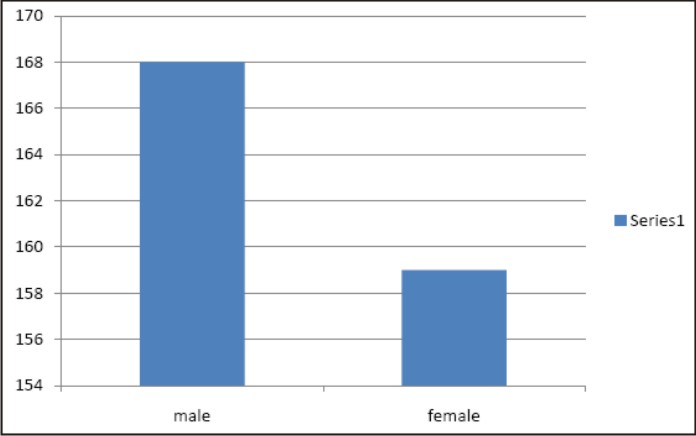 | Fig 1 : Prevalence Of Traumatic Dental Injuries According To Gender
 |
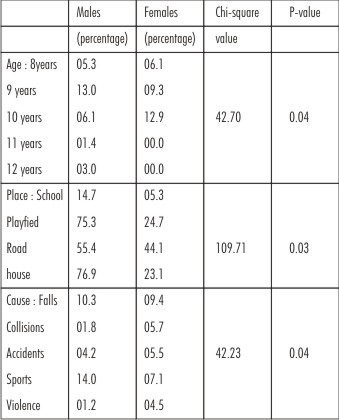 | Table 1 : Percentage Among Males And Females Of Different Variables.
|
There was maximum incidence of Ellis classIII fractures in males while in females Ellis Class II type of tooth fractured dominated (Figure2). On analyzing the place where maximum injuries occurred, males suffered maximum amount of TDI at home followed by playfields, road and schools whereas in females maximum trauma was seen in playfield (Table1). Fall was found to be the major causative factors of trauma in females and sports was the main factor in case of males (Table 1).
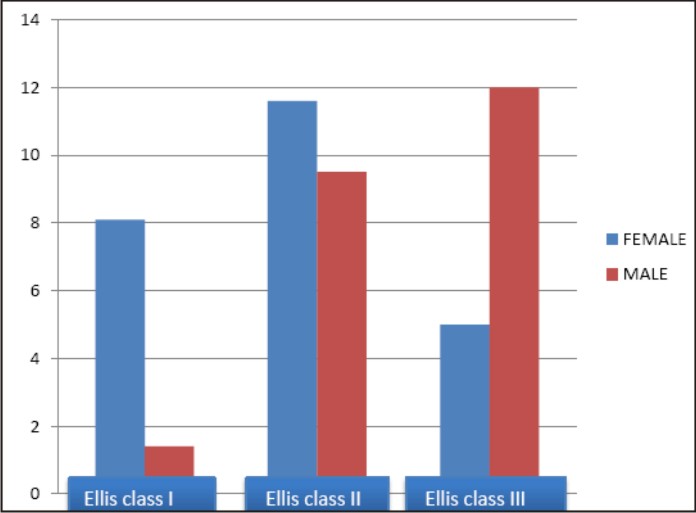 | Fig 2 : Most Common Type Of Traumatic Dental Injury In The Examined Children (Percentage)
|
Discussion
Dental trauma refers to injury of the teeth or the periodontium and the nearby soft tissues such as lips, tongue etc. These injuries tend to occur more at a young age when growth and development is taking place[9].Trauma has great impact on the quality of life of the child.On an average, children with an untreated TDI were 20 times more likely to report an impact on quality of life when compared to children without a TDI[10], [11].
In various studies, a wide range of prevalence levels of TDI have been seen because they have different diagnostic criterias, methodologies and populations. Prevalence refers to all the cases of TDI new or old, in a population at a given time [12]. The present study showed a prevalence of 27.8%, showing increased risk of TDI in Himachal population .The results were similar to the study conducted by Prabhu et al [13] in which the prevalence of TDI was 23.8%. Studies done by Ravishankar [14] in South India and Sharma and Dua[15] in Punjab showed comparatively less prevalence of 15.7% and 14.5% respectively.This can be attributed to the difficult and mountainous terrain lacking playgrounds for children in Himachal Pradesh.According to Ravn[16], however, one study cannot be compared with another study of dental trauma.
Greater amount of trauma was observed in boys (29.4%) than in girls (28.4%), but the difference was marginal. A similar study carried out by Garcia - Godoy et al[17] also showed a small difference between trauma prevalence in boys and girls.This can be due to the increased participation of girls in sports and other vigorous activities. Traebert et al[18] also explained in his study that girls can be exposed to the same TDI risk factors as boys, which is characteristic of modern western society.Thus, it is probably the activities of a person and the environment in which he resides which act as the determining factors of TDI than the gender.
Age is another well known risk variable. School children and teenagers are the target groups, but less has been documented about very young children. Results from many studies [19], [20], [21], [22] affirmed that the majority of TDI’s occur in children and adolescents. It is estimated that about 71-92% of all TDI’s sustained in a lifetime occur before the age of 19 years. Other studies [23], [24] reported a decrease in TDI after the age of 24-30 years. In the present study, 13% of TDI was seen in 9 year males and 12.9% of TDI was observed in 10 year females, which was similar to the study done by Marcenes et al [25] in 9-12 year old Syrian children.This is due to the fact that children are more active during this age and they lack motoric coordination. For this reason they are unable to precisely evaluate the danger associated with velocity. As they grow, their risk towards TDI is reduced.[26]
In the present study, prevalence of Ellis class II fractures was most common (10.3%) followed by Ellis class III type of tooth fracture (8.8%). This was consistent with the findings in the United Kingdom survey[27] and with the reports of several other authors [28], [29], [30].These complicated types of dental fractures require immediate dental care with close review and adherence to follow up appointments, to reduce the complications associated with delayed treatment.
Our study showed schools to be the most common place of injury followed by playfields.This is due to the fact that children spend around 60% of their time at their homes under the care and supervision of their parents, thus the prevalence of trauma at home was less. The only time children lack supervision was at school, this was validated by Gupta et al[31] in their study in South Kanara. The schools, thus, act as an ideal setting where children meet their peer groups and get involved in physical activities unattended.
Due to increased participation in sports and other vigorous activities by children, sports account for the prime cause of TDI with a prevalence of 10.6%, followed by falls with an incidence of 9.4% in the present study. Similar result was found by Prabhu A, et al [13] in a study conducted on 458 children of sainik school, where TDI due to sports was seen to have a prevalence of 62%.The present study also reported an increase in sports related injuries (7.1%) amongst females, due to the increased participation of females in sports [6],[7],[8] as a result of increased awareness.This corroborates the results of studies conducted by Marcenes et al [25] and Nicolau et al [32]. Thus, societal changes account for this increased incidence of trauma among females.
Conclusion
The increasing incidence of TDI, which has become a social health problem, needs immediate intervention. Improvement in the physical environment of children, along with close supervision when they are involved in physical activities is likely to have a positive impact in reduction of TDI. Screening camps can be conducted at schools to identify children at high anatomic and behavioural risk of trauma, followed by appropriate intervention through orthodontic treatment. Also, increasing awareness about TDI and its effective management and adoption of health policies will help reducing the increasing traumatic dental injuries.
References
1. Andreason JO, Andreason FM Textbook and color atlas of traumatic injuries to teeth, ed3.Copenhagen.Munksgaard publishers,1994.
2. Hamilton FA, Hill FJ, Holloway PJ. An investigation of dentoalveolar trauma and its treatment in an adolescent population. Part I:the prevalence and incidence of injuries and the extent and adequacy of treatment. Br Dent J 1997;182:91-95
3. Burton J, Pryke L, Rob M, Lawson JS. Traumatized anterior teeth amongst high school students in Northern Sydney. Aust Dent J 1985; 30:346-348
4. Gutmann JL, Gutmann MS. Cause, incidence and prevention of trauma to teeth. Dent Clin North Am 1995;39:1-13.
5. Noriah N, Hussein Nik. Traumatic injuries to anterior teeth among schoolchildren in Malaysia. Dental Traumatology2001; 17:149-152
6. Burden DJ.An investigation of the association between overjetsize. Lip coverage, and traumatic injury to maxillary incisors. Eur J orthod 1995:17:513-7
7. Rocha MJ, Cardoso M. Traumatized permanent teeth in Brazilian children assisted at the Federal University of Santa Catarina, Brazil. Dent traumatology 2001; 17:245-9
8. Traebert J, Peres MA, Blank V, Boell RD, Pietruza JA. Prevalance of traumatic dental injury and associated factors among 12-years-old school children in Florianopolis, Brazil.Dent Traumatol2003;19:15-8.
9. Andreason J, Andreason F and Andersson L. Textbook and colour Atlas of traumatic injuries to teeth fourth edition
10. Soriano EP, CaldosJr AF, Carvalloh MV, AmoriumFilho HA. R32;Prevalence and risk factors related to traumatic dental injuries R32;in Brazilian school children. Dent Traumatol 2007;23:232-40.
11. Cortes MIS, Marcenes W, Sheiham A. Impact of traumatic injuries to the permanent teeth on the oral health-related quality of life in 12-14 yeae old children. Community Dent Oral Epidemiol 2002:30:193-8.
12. Glendor Ulf. Epidemiology of traumatic dental injuries- a 12 year review of the literature. DentTraumatology 2008;24:603-61.
13. Prabhu A, Rao AP, Govindarajan M, Reddy V, Krishnakumar R, Kaliyamoorthy S. Attributes of dental Trauma in a school population with Active sports involvement. Asian J Sports Med 2013;4(3):190-194
14. Ravishankar TI, Kumar MA, Ramesh N,Chaitra TR. Prevalence of Traumatic Dental Injuries to permanent Incisors among 12-year old school children in Davangere, South India.The Chinese Journal of Dental Research 2010;13(1).
15. Dua R, Sharama S. Prevalence, cause and correlates of traumatic dental injuries among seven to twelve year old school children in Dera Bassi.www.ncbi.nlm.nih.gov/pmc/articles/ PMC3341757
16. Ravn JJ. Dental injuries in Copenhagen school children, school years 1967-1972. Community Dent Oral Epidemiol 1974; 2:231-45.
17. Garcia-Godoy F, Morban-Laucer F, Crominas I.R, Franjul RA, Noyola M. Traumatic dental injuries in school children from Santo Domingo. Community Dent Oral Epidemiol 1985;13:177-9
18. Traebert J, Bittencourt DD, Peres KG, Peres MA, De Lacerda JT, Marcenes W. Aetiology and rates of treatment of traumatic dental injuries among 12-year-old school children in a town in southern Brazil. Dent Traumatol 2006;22:173-8
19. Glendor U, Haling A, Andersson L, Eilert-Petersson E. Incidence of traumatic tooth injuries in children and adolescents in the county of Våstnanland, Sweden. Swed Dent J 1996;20:15-28.
20. Davis GT, Knott SC. Dental trauma in Australia. Aust Dent J 1984;29:217-21
21. Ianetti G, Maggiore C, Ripari M, Grassi P. Studio statistic sulle lesion traumatichedeidenti. Minerva Stomatol 1984;33:933-43. In Italian
22. Redfors Å, Olsson B. TandskadorinorraÅlvsborg 94020195013: en delstudie I “Skaderegistreringen I NorraAlvsborg”. Vånersborg: LandstingetiÅlvsborg: 1996. In Swedish
23. Shulman JD, Peterson J. The association between incisor trauma and occlusal characteristics in individual 8-50 years of age. Dent Traumatol 2004;20:67-74
24. Holland TJ, O’Mullane DM, Whelton HP. Accidental damage to incisor amongst irish adults. Endod Dent Traumatol 1994;10:191-4
25. Marcenes W, Al Beiruti N, Tayfour D, Issa S. Epidemiology of traumatic injuries to the permanent incisors of 9-12- year-old schoolchildren in Damascus, Syria. Endod Dent Traumatol 1999;15:117-123
26. IvancicJokic N, Bakarcic D, Fagosic V, et al. Dental trauma in children and young adults visiting a University Dental Clinic. Dent Traumatol 2009; 25:84-7
27. O’Brien M. children’s dental health in the United Kingdom 1993. OPCS. London: HMSO; 1997.
28. O’Mullane DM. Some factors predisposing to injuries of permanent incisors in school children. BR Dent J 1973;134:328-32.
29. Macko, DJ, Grasso JE, Powell EA, Doherty NJ. A study of fractured anterior teeth in a school poplation. ASDC J Dent Child 1979;46:130-3
30. Hamdan MA, Rock WP. A study comparing the prevalence and distribution of traumatic dental injuries among 10-12 years –old children in an urban area of Jordan. Int J paediatrDent 1995;5:237-41
31. Gupta K, Tandon S, Prabhu D. Traumatic injuries to the incisors in children of South Kanara district. A prevalence study. J Indian SocPedodPrev Dent 2002;20:107-13
32. Nicolau B, Marcenes W, SheihamA.Prevalence, causes and correlates of traumatic dental injuries among 13-year-olds in Brazil. Dent Traumatol 2000;17:17-21
|