Introduction
Most of the complete denture patients find it difficult in carrying out functional activities such as mastication and speech due to their inability to control the dentures effectively. Loss of teeth leads to changes such as resorption of alveolar ridge, tongue expansion, loss of tonicity of facial muscles, reduction of lower face height, loss of vertical dimension of occlusion, anterior rotation of the mandible, increase in relative prognathia, changes in inter-alveolar ridge relationship, sharp, spiny, uneven residual ridges, resorption of the mandibular canal wall, location of the mental foramina close to the top of the mandibular residual ridge. This provides serious problems to the clinician on how to provide adequate support, stability and retention of the denture. For this reason, it is critical when constructing complete dentures to incorporate features that will aid in stability during function. In 1933, Sir E. Wilfred Fish introduced the concept of Neutral zone. Neutral zone is defined as “that area in the mouth where the forces of tongue pressing outward are neutralized by forces of cheeks and lips pressing inward. This concept is also termed as Reciprocal space, potential space, denture space, reciprocal zone, Zone of minimal conflict, Zone of neutral muscular force[1]. During fabrication of the complete denture the position of the teeth and the external surfaces of the denture should follow the Neutral zone so that the forces exerted on the denture are neutralized [2]. With resorbed ridges, the vectors of force that are transmitted through anatomic cusps will dislodge the lower denture hence Linear occlusion scheme was designed. In this scheme mandibular cuspless teeth occludes with maxillary anatomic teeth that have been modified (bladed teeth) in order to achieve Linear occlusal contacts which provides a stabilizing effect on the denture bases during function [3],[4]. Failure to recognize the importance of tooth position and flange contour often results in dentures which are unstable and unsatisfactory even though they are skillfully designed and expertly constructed [5].
Case Presentation
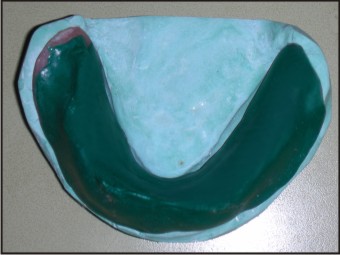
A female patient aged 47yrs came to the department of prosthodontics, with the complaint of missing teeth in the maxillary and mandibular arch and wanted an replacement withnew denture. History revealed she was edentulous since 4 yrs. On intraoral examination - Atwood's class v mandibular ridge, Ridge relation - class I, Interarch space was adequate, Frenal and muscle attachment close to the crest,tongue was slightly enlarged and partially extending onto the ridge. (Fig.1).
 | Figure 1: Resorbed Mandibular Edentulous Ridge.
 |
Treatment Planning
Removable complete denture prosthesis was planned using Neutral zone technique for mandibular ridge and Linear occlusion. Ridge augumentation and implant procedure were ruled out as the patient refused to undergo any surgery.
Treatment Objectives
1) to rehabilitate the patient with complete denture prosthesis.
2) to preserve the remaining residual ridge.
3) to locate the Neutral zone for teeth arrangement and to contour the denture base.
4) to attain maximum stability,comfort and function.
5) to incorporate extremely efficient chewing mechanism with Linear occlusion [4],[6]
Primary impression for maxilla was made using impression compound.mandibular impression was made using alginate (mucostatic impression technique). Primary casts were poured with type II gypsum. Maxillary border molding and secondary impression was made, master cast was poured with dental stone. Maxillary denture base and occlusal rim were prepared . Maxillary rim was adjusted for proper esthetics, occlusal plane, phonetics and lip support . Midline, canine line, high lip lines were marked.Mandibular custom tray was a plate of acrylic, without the handle. Three vertical stops of acrylic were adapted over the special tray.These stops were joined by a wire bent in a sinusoidal manner extending from molar to molar. (Fig.2) Mandibular custom tray overextension and stability was checked. The patient was trained properly for various functional movements before inserting the tray. Two occlusal pillars were then built up with green stick compound on opposite sides of the lower arch. These pillars were moulded and adjusted to achieve 3mm freeway space and establish the correct vertical dimension. Green stick compound was softened and loaded on the mandibular tray and inserted into patient’s mouth. Patient was instructed to do functional movements like sucking, swallowing, smiling, pursing of the lips, slightly protruding the tongue and licking the lips. These actions were repeated for 10 minutes until material got set. With these actions the greenstick compound gets molded between the lip and the tongue in the anterior region and cheek and lateral border of the tongue in the posterior region into the region of Neutral zone. (Fig. 3) These movements recorded a greater detail of action of lips, cheeks and tongue and also determined the thickness, contours and shape of polished surface of denture. The compound was reheated in water bath and the procedure repeated to confirm the shape of Neutral zone. After the vertical dimension and centric relation had been established, the final impression was made with closed-mouth procedure. (Fig. 4) Only after the final impression was made the centric relation was sealed.
 | Figure 2: Mandibular Custom Tray With Metal Spurs That Acts As Retentive Components For The Impression Material.
|
 | Figure 3: Greenstick Compound Molded As Per Patient’s Neutral Zone.
|
 | Figure 4: Recording Of Centric Relation And Final Impression (Close-mouth Impression Procedure).
|
The Plaster Index
Final impression was poured with dental stone. Before the stone set completely two notches were made in the lingual center section, and the other two were made on each of the buccal side, one in the cuspid and one in the molar region. (Fig. 5) Separating medium was applied all over the base. The green stick compound and the notches were covered with plaster in two sections, leaving a narrow dividing line of the compound at the occlusal and incisal edges of the pattern so that the lingual and buccal sections of the plaster index did not meet. After the plaster was set, the buccal and labial portions were removed in two sections. The lingual portion was removed as a single piece. The shape of the Neutral zone was permanently registered in the plaster index. (Fig.6). The greenstick compound was softened and disposed. The plaster index was then coated with a separating media and assembled with the acrylic denture base in position. The red baseplate wax was slowly melted in an enamel bowl and poured into the plaster index through the space between the labial and lingual indices on the occlusal surface. (Fig. 7) When the plaster index was opened, Neutral zone recorded with greenstick was replaced by wax. Thus both the upper and lower occlusion rims were formed. Teeth were then be set up following the index.
 | Figure 5: Mandibular Master Cast Indexed With Two Notches In The Lingual Center And Two On Each Of The Buccal Sides.
|
 | Figure 6: The Shape Of The Mandibular Compound Rim Captured With Buccal And Lingual Plaster Indices.
|
 | Figure 7: Wax Rim Located In The Neutral Zone.
|
Teeth Arrangement In Linear Occlusion:
Zero degree (monoplane) teeth were arranged in the maxilla opposed by bladed teeth in the mandible. The blades of the bladed teeth were in a precisely straight line over the crest of the ridge. There was no anterior tooth interference in protrusive or lateral movements. A Clinical wax try-in was done and checked for esthetics, phonetics and occlusion. Dentures were cured, finished, polished and inserted (Fig.8). The mandibular denture was checked for stablity with all the movements of the lips, cheeks and tongue. Post insertion instructions were given and the patient was recalled for checkup.
 | Figure 8: Denture Insertion.
|
Discussion
When the residual alveolar ridges have resorbed significantly denture stability and retention are more dependent on correct position of teeth and contour of the external surfaces of the dentures[7]. Hence the concept of Neutral zone philosophy and Linear occlusion and was advocated in this case report. The Neutral zone philosophy is based upon the concept that for each patient there exists within the denture space a specific region where the function of the musculature during chewing, speaking, swallowing and various other functional activities of the mouth will not unseat the dentures and where inward forces exerted by lips and cheeks, and outward forces exerted by tongue are in equilibrium [2],[6]. while recording this zone the internal and external muscle groups become activated, moving them through their respective action paths. With this activation,the reciprocating pressures from the muscles are exerted upon the compound, which gradually gets molded into a state of neutral balance and becomes centrally inert in relation to all of the complex forces acting upon it [5]. This technique provides a more stable and retentive mandibular complete denture with resorbed ridges. Greater comfort and improved speech clarity. Shorter treatment time as compared to conventional denture as bordermolding, final impression and jaw relation are completed in one appointment, more harmony with surrounding perioral musculature[1],[8]. Many materials have been suggested for this technique such as: impression compound, soft wax, silicone and tissue conditioners and resilient lining materials. In this case modeling green stick compound was found to be better than tissue conditioner to locate the Neutral zone, as the later sets gradually patient could not maintain the same position till the material sets. Due to its tackiness in tissue conditioner it was difficult to manipulate. Neutral zone formed with tissue conditioner is narrower posteriory thus limiting premolar and molar positioning[9]. In 1966 J.P. Frush described occlusion in geometric terms as one-dimensional (linear), two dimensional(flat plane), and three-dimensional(cusped). This classificationof occlusionspecifically classified the dimensional contactbetween occluding posterior teeth.In linear occlusion, the arch requiring the greatest stability may determine the archreceiving the bladed teethwhich is most often the mandibular arch.The occluding forces with linear occlusion are vertical in centric and eccentricpositions .The location offorce onthe mandibular edentulous ridge does not vary regardless of the occluding position.There is minimal surface contact area between theflat plane and bladed teeth thus denturebase movement is minimized. Since there is no anterior tooth interference in protrusive or lateral movementsprovidesa consistent vertical seating force in both centric and eccentric movement; hence, transverse force vectors are minimized.[3] In this case Linear occlusionwas chosen as the occlusal scheme to increasethe stability of denture bases by minimizing the lateral forces applied to the denture base.
Conclusion
With Neutral zone technique and Linear occlusion patients did report greater comfort and improved speech clarity. Exceptional mandibular denture stability due to lack of movement of the denture bases and fewer postoperative appointments compared to conventional denture could be achieved.
References
1. Pawah S, Gupta A, and Madan B.The relation of the Neutral zone to the crest of the residual alveolar ridge in completely edentulous subjects-A clinico-Radiological study. Journal of Oral Health and Community 2011;5:90-93
2. Beresin VE and Schiesser FJ. The Neutral zone in complete dentures. J Prosthet Dent 2006;95:93-101
3. Williamson RA, Williamson AE, Bowley J and Toothaker R. Maximizing mandibular prosthesis stability utilizing Linear occlusion, occlusion plane selection, and centric recording. J Prosthodont 2004;13:55-61
4. Frush JP. Linear Occlusion. Cited from www.geneva-dental.com/pdf/Linear%20Occlusion.pdfaccessed on 25/8/2012
5. Chandrashekar S. Management of a severly resorbed mandibular ridge with the Neutral zone technique. Contemp Clin Dent 2010;1:36-39
6. Gupta KL and Agarwal S.Salvation of a severly resorbed mandibular ridge with a Neutral zone technique. Ind J Dent Res 2011;22:883
7. Sheldon W and Douglas AA. The problems of reduction of residual ridges.In: Essentials of complete denture prosthodontics.Ishiyaku EuroAmerica,Inc.Publishers, 1996; pp 22-38
8. Wee AG, Cwynar RB and Cheng AC. Utilization of the Neutral zone technique for a maxillofacial patient. J Prosthodont 2000;9:2-7
9. Makzoumé JE. Morphologic comparison of two Neutral zone impression techniques: A pilot study. J Prosthet Dent 2004;92:563-8
|