Introduction
A fibrous or flabby ridge is a superficial area of mobile soft tissue affecting the maxillary or mandibular alveolar ridges. It can develop when hyperplastic soft tissue replaces the alveolar bone and is a common finding, particularly in the upper anterior region of long term denture wearers.
Various reasons have been cited for the development of flabby tissue, these include complete maxillary denture opposing natural mandibular anterior teeth and partial denture[1], not removing denture during night, dentures constructed with anterior porcelain teeth and posterior resin teeth, badly constructed dentures such as loose ill-fitting dentures as well as dentures with wrong centric occlusion relation, occlusal disharmony and traumatic occlusion.
Displaceable or flabby ridges present a particular difficulty when making complete dentures. Unless managed appropriately, such flabby ridges adversely affect the support, retention & stability of complete dentures.[2] Published studies indicate that the prevalence of flabby ridges can vary, occurring in upto 24% of edentate maxillae and in 5% of edentate mandibles.[3],[4]
Clinical Report
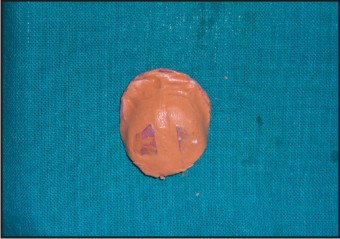
A 64 year old edentulous female sought treatment at the Prosthodontic Department in Subharti Dental College, Meerut, for prosthetic rehabilitation. On clinical examination, patient was found to be complete edentulous. It was noted that there was an extensive area of flabby tissue present on the anterior region of her maxillary denture bearing areas [Figure:1].
 | Fig 1: Flabby Ridge In Maxillary Anterior Area
 |
History revealed that the patient was an old denture wearer and did not remove the denture at night. On examining the old denture, it was found that the teeth were attrited and the denture was not retained well in mouth. There was no suggestive history of diabetes, high blood pressure or any other systemic disease.
Following discussion with the patient regarding available treatment options, it was clear that she was very apprehensive regarding procedures such as surgical removal of flabby ridges, bone grafting or placement of dental implants due to her age, long treatment time and high cost ,so she wanted to avoid these procedures. Therefore, it was decided to fabricate a new complete denture, through modified impression technique - palatal splinting using two part tray system.
Procedure
Preliminary impressions for both dental arches were obtained with a low viscosity irreversible hydrocolloid impression material (Imprint, 3M ESPE, Germany) to ensure minimal distortion of the flabby tissue. The impressions were poured in Type III dental stone (Kalstone, Kalabhai Karson, Mumbai) to obtain the primary casts. The displaceable areas were identified on the maxillary cast.
Single uniform thickness of modelling wax (Y Dents, MDM Corporation, Delhi) was placed as a spacer over the identified displaceable area on the maxillary cast [Figure:2]. Palatal tray was fabricated with the autopolymerizing acrylic resin (DPI RR cold cure, DPI, India) and over it three stops of acrylic were made [Figure:3]. Then, the custom tray was fabricated over the palatal tray [Figure:4]. The three acrylic stops allow the custom tray (second special tray) to be guided in an oblique upward and backward direction to envelope the palatal tray (first tray).
 | Fig 2: Wax Spacer Over Flabby Area
|
 | Fig 3: Palatal Tray With Acrylic Stops
|
 | Fig 4: Custom Tray Envelop Palatal Tray
|
Border molding was done with low fusing compound (DPI Pinnacle tracing sticks, DPI, India) in the custom tray [Figure:5]. Then, wax spacer was removed from the palatal tray and an impression was made with zinc-oxide eugenol impression paste (DPI impression paste, DPI, India) [Figure:6]. When this impression was set, the final impression was made in the custom tray using medium body addition silicone (Aquasil Ultra Monophase, Dentsply, USA) with the palatal tray impression in place over the flabby ridge [Figure:7]. The presence of zinc-oxide eugenol impression paste in palatal tray prevents backward displacement of the mobile ridge when the custom tray was inserted in backwards & upward direction.
 | Fig 5: Border Molding In Custom Tray
|
 | Fig 6: Palatal Tray With Final Impression
|
 | Fig 7: Custom Tray With Final Impression
|
For mandibular ridge custom acrylic resin tray was fabricated and border molding was done with low fusing compound and final impression was made using zinc-oxide eugenol impression paste. Both the impressions were poured with Type III dental stone to obtain master cast. Jaw relation records were made with the occlusion rims oriented to the established vertical dimension of occlusion, the anatomic occlusal plane, and the patient’s centric relation. After teeth arrangement, try-in was carried out. The denture was cured using heat cure acrylic resin (DPI-heat cure, DPI, India) in the conventional manner. Then, it was finished & polished and was ready to be delivered to the patient. During insertion of the complete denture, it was checked for border extension, proper adaptation and occlusion [Figure:8]. Home care instructions (oral hygiene instruction, insertion & removal of prosthesis) were imparted to the patient and routine follow-up appointments were scheduled.
 | Fig 8: Denture In Occlusion
|
Discussion
There are varieties of treatment options available for the management of flabby ridges, one is multitude of impression technique to record a suitable impression of a flabby denture bearing area.
Lidddlelow[5] described a technique whereby two separate impression materials are used in custom tray. Watson[6] described the window impression technique where a custom tray is made with a window or opening over the flabby tissue. Allan Mack described splint method in which plaster is used to record an impression of flabby tissue and when it becomes set, same material is used to record the full arch impression.[7]
Using the palatal splinting technique it is conceivable that a minimal degree of distortion occurs when upward force is maintained in first stage of impression and second stage of impression prevents backward displacement of the mobile ridge.
Other treatment modalities include surgical debulking of the flabby tissue, it would result in shallow ridge & it may provide little retention or resistance to lateral forces on the resultant denture. One is reminded of the concept that prosthodontic therapy should be considered with the conservation of what remains, rather than the meticulous replacement of what has been lost.[8] Implant retained prosthesis may offer a solution to the problem of stability & retention but they are not without their disadvantages i.e surgery, treatment time, cost, etc.
Conclusion
There are a variety of impression techniques available to address the problem caused by the unsupported tissue. This paper has described a modified impression technique - palatal splinting using two part tray system. The denture with this modified impression technique brought about sufficient masticatory efficiency and denture stability and resulted in patient satisfaction [Figure 9]. The materials used in this technique are readily available and are used in contemporary dental practice. This technique does not require additional clinical visits & cause minimal discomfort to the patient as compared to other treatment modalities for displaceable tissues.
 | Fig 9: Post Rehabilitation Photograph
|
References
1. Kelly E: Changes caused by mandibular partial denture opposing a maxillary complete denture. J Prosthet Dent 1972; 27: 210-215.
2. Basker RM, Davenport JC: Prosthetic treatment of the edentulous patient. 4th ed. Oxford: Blackwell 2002.
3. Carlsson GE: Clinical morbidity and sequelae of treatment with complete denture. J Prosthet Dent 1998; 79: 17-23.
4. Xie Q, Nahri TO, Nevalaineeu JM et al: Oral status and prosthetic factors related to the residual ridge resorbtion in elderly subjects. Int J Prosthodont 1997; 55: 306-313.
5. Liddelow KP: The prosthetic treatment of the elderly. Br Dent J 1964; 117: 307-315.
6. Watson RM: Impression technique for maxillary fibrous ridge. Br Dent J 1970; 128: 552.
7. Lynch CD and Allen PF: Management of the flabby ridge: using contemporary materials to solve an old problem. Br Dent J 2006; 200: 258-261.
8. Devan MM: The nature of the partial denture foundation: suggestions for its preservation. J Prosthet Dent 1952; 2: 210-218.
|