Introduction
Crown fracture has been documented to account up to 90% of all traumatic injuries to the permanent dentition. Many epidemiologic studies show that most dental injuries involve just one tooth and maxillary incisors are the most commonly affected[1],[2]. It has been reported males are more frequently affected than females, particularly in the maxillary incisors[3]. An alternating treatment option for restoring fractured incisors is using bonding agent for the chipped fragment onto the natural crown. The first published case of reattaching a fractured incisor fragment was reported in 1964 by Chsuck A et al.[4] when clinicians described a case of rehabilitation of a fractured incisor using the patient’s original tooth. After this many articles have been published regarding a variety of preparations designs and materials for reattachment. Many clinicians published articles for fragment and tooth preparation, using an acid etch technique and composite technique[5]. Introduction of new dentine bonding agent available, fragment reattachment is becoming more attractive and the introduction of fiber posts by Duret et al. in 1990 offered anaesthetic solution for the restoration of traumatized teeth. Uncomplicated crown fractures can be treated according to the extent of hard tissue loss with enamel recontouring, composite bonding, or porcelain veneers. Due to the reflection of metal shade through the remaining tooth structure, these posts present some aesthetic concerns[6],[7],[8],[9].
The educational attempts of dental professional regarding trauma have resulted in patients presenting with intact avulsed teeth, as well as fractured coronal tooth fragments. If an intact tooth fragment is present after trauma, the incisal edge reattachment procedure presents a conservative, simple and aesthetic alternative[6]. The advantages from reattachment of fractured tooth fragment are[6],[7],[8]
a) Reduced chair-side appointments.
b) Psychological acceptance by the patients and parents.
c) Accurate restoration of tooth morphology and texture, and using the natural tooth, the abrasion would be similar to that of the contralateral and opposing teeth,
d) Colour matching,
e) Wear similar to adjacent and opposing tooth,
f) Good aesthetics,
g) Preservation of incisal translucency,
h) Economical,
i) Preservation of occlusal contacts,
j) Colour stability of enamel,
The objective of this case report is to present the reconstruction of a traumatized and fractured right maxillary lateral incisor by building a composite resin core with a glass fibre post.
Case Report
A 26 year old patient sought treatment at Department of Conservative and Endodontics, after he sustained a crown fracture in the permanent maxillary right lateral incisor. A complete history of the incident was noted and then an elaborate clinical examination of the tooth and rest of the dentition were carried out. Ellis Class 111 fracture of right upper lateral Incisor was observed (Fig 1a) and the patient was more concerned about immediate restoration of aesthetics. Therefore we decided to restore aesthetics immediately by reattaching the original crown fragment after ruling out periodontal damage, root fracture and bony fracture. To prevent dehydration the original tooth fragment was kept in Hanks balanced salt solution (HBSS) till the completion of root canal treatment (Fig 1b). Pulp vitality was checked thermally (sensitivity to cold stimulus) and confirmed with positive responses.
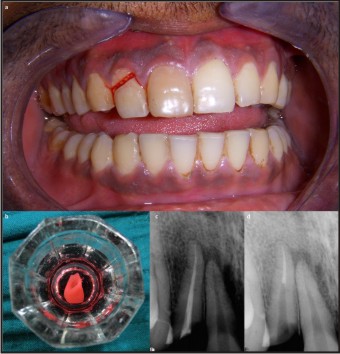 | Figure 1: The Preoperative photograph showing fractured crown in position (a). The extracted crown fragment placed in the HBSS solution (b). The radiograph immediately after obturation of root canal (c) and after space prepared for post placement (d).
 |
Subsequent to this, an intraoral periapical radiograph (IOPA) of 12 region was taken. The IOPA revealed pulpal involvement. The coronal fragment resembled a laminate veneer, and its cervical margin was slightly sub-gingival. No alterations in the periodontal and bone tissues were observed in the radiographic examination. As the first clinical step, the coronal fragment and remaining root portion were cleaned with rubber cup pumice prophylaxis. After completing the endodontic treatment (Fig 1c) and post space preparation was done (Fig 1d) in the coronal fragment as well as in the root canal for proper retention of the fractured fragment assembly. Glass fibre post was selected as the patient was concerned more about his aesthetics. The coronal fragment and remaining root portion were then etched with 37% phosphoric acid (Fig 2a), rinsed thoroughly, and gently air-dried. The coronal fragment was re-attached to the root remnant using an adhesive restorative technique with an etch-and-rinse adhesive system (Fig 2b) and a light-cured micro hybrid composite resin (Fig 2c) was spun into the root canal and the glass fibre post seated (Fig 2d) and cured (Fig 2e).
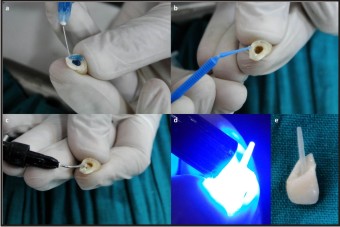 | Figure 2: The fractured portion of the crown fragment being conditioned with 37% phosphoric acid gel (a), application of bonding agent (b), placement of resin composite (c), curing of the composite with fiber-post in position (d) and finally the cured pos
|
Simultaneously, the coronal tooth fragment was placed into the stent, its bonding surface and pulp cavity loaded with dual cure cement. This was placed into position and held until the cement was light cured set (Fig 3). All restored surfaces were finished with fine-grain diamond points and polished with fine and superfine grain polishing discs. Antibiotic therapy (amoxicillin 500 mg, 3 times / day) was started and maintained for 5 days. The use of 0.12% chlorhexidine oral rinse twice daily for 7 days was prescribed. After 15 days, a groove extending from the buccal to the palatal side of the tooth was prepared with a No. 1302 round diamond bur at high speed along the fracture line and was restored with composite resin in order to mask the union between the fragments and improve aesthetics. Follow-up after 6 months showed good adaptation of the tooth fragment/composite resin restoration, pulpal vitality, no signs of root resorption, and no painful symptoms (Fig 3e).
 | Figure 3: The application of etchant on the fractured tooth inside the mouth (a), application of bonding agent (b), fiber-post with crown assembly together luted in the root canal (c), curing of luted cement (d), and the final postoperative labial view (e
|
Discussion
Traumatized anterior teeth require quick repair for both functional and aesthetic needs. By using the original tooth fragment to restore a fractured tooth, it is possible to achieve a very good aesthetics. Traumatic injuries involving tooth fracture can be treated by reattachment of the tooth fragment using a dentine adhesive system to provide what is considered to the most conservative to restoration. The traditional conservative treatment of crown fractures has been restorations with composite resin and a dental bonding system. Newer dentine bonding systems work well with such efficiency that they easily allow for normal masticatory forces. Adhesive systems can now be used to treat tooth fractures by reattachment of the tissue fragment to provide best restoration.
Factors influencing the extent and feasibility of such repairs include the site of fracture, size of fractured remnants, periodontal status, pulpal involvement, maturity of root formation, biological width invasion, occlusion and time. The fractured fragment needs to be preserved in sterile saline or water or HBSS to prevent color change due to dehydration of the tooth. Dehydrated fractured fragment might get rehydrated over few months. Survival rates for such restoration have been shown to the good with failure often only resulting from repeated trauma[10]. If the fracture involves two-third or more of the crown a post - reattachment is more commonly used.
The composite reinforcement technique together with this light-transmitting post had been widely used to functionally and aesthetically restore compromised root filled teeth[11]. Restoration with a post after endodontic treatment provides retention of a core to support coronal restoration especially with extensive tooth loss. Traditionally, these posts have been cast or machined from metals, and can be grouped as active or passive posts[12]. Active posts derive their primary retention directly from the root dentine by the use of threads. Passive posts rely primarily on luting cement for their retention.
The present case report indicated that reattachment of fractured incisal fragments by using new generation bonding agents was effective. The advantages of using the original tooth fragment over other materials include better color match, morphology, translucency, patient acceptance and economical[13]. If the fracture involves two thirds or more of the crown a post-reattachment was more commonly used. Post placement was also to be considered in fractures where the patient exhibits a large over jet and/or para-functional habits Post placement in addition to bonding, serves to retain the coronal portion via a friction bond, and assists in preventing dislodgement from non-axial forces. It is acknowledged that the placement of traditional metal posts weakens the roots and leads to root fracture, or may lead to caries that may cause irreversible failure and extraction of tooth in some cases[14],[15].
According to the findings of finite element analysis of stresses in endodontically treated teeth restored with posts, flexible glass post systems gave the most stressing condition as compared to carbon or steel posts[16]. In a retrospective study of the clinical performance of 1314 placed fibre posts, the survival rate was 96.8%[17]. For the treatment of the present case, a composite core was built up over the fibre post to provide aesthetically pleasing temporary restoration to the patient. The composite core build up used in this case enabled the placement of a bracket to the tooth. Some of the disadvantages of reattachment includes: the necessity for continuous monitoring, its unknown longevity, and possibility of color changes of the bonded fragment[18]. Other treatment options which are available have associated limitations like multiple visits, stabilization and are less conservative in nature. Adhesive tooth fragment reattachment may provide good results on a short - and medium-term basis[19]. However, dehydration of the fragment when it remains dry after the accident is a major problem with this technique. Dentists should teach their patients about the importance of collecting fragments of teeth damaged due to traumatic injuries. They should provide instructions on the use of an adequate wet storage medium, so that the fragments can be suitable for reattachment.
In the present case, the fragment was maintained in the oral cavity since the accident, which avoided desiccation and color change. Our case was followed up for six months without noticeable color change of the crown or periapical radiological changes. The patient continued with the reattached fragment as a permanent restoration. Preparation of ceramic/porcelain fused to metal (PFM) restoration requires multiple visits, tooth preparation and laboratory procedures. Hence we recommended that the original reattached fragment be allowed to continue as permanent restoration unless tooth exhibits color changes or there is subsequent trauma[13],[20]. Limitations of tooth tissue reattachment include those associated with dental adhesion restorative cement in particular control of operating field from contamination and force application, particularly indirect or shear forces working in directions where bonding forces are weakest.
Conclusion
Reattachment of the intact fractured segment can be considered as an ultraconservative method for aesthetic rehabilitation. Reattaching a tooth fragment with the superior quality adhesive materials make this procedure viable. This procedure helps us to preserve maximal natural tooth structure. The need of the day is to educate the public to preserve the fractured segment and seek immediate dental treatment.
Acknowledgement
We would like to thank all the staff members from Departmentof Conservative and Endodontics, for their support & cooperation.
References
1. Shulman JD, Peterson J. The association between incisor trauma and occlusal characteristics in individuals 8–50 years of age. Dent Traumatol 2004;20:67–74.
2. Caliskan MK, Turkun M. Clinical investigation of traumatic injuries of permanent incisors in Izmir, Turkey. Endod Dent Traumatol 1995;11:210-3.
3. Rapelli G, Massaccesi C, Putignano A. Clinical procedures for the immediate reattachment of a tooth fragment. Dent Traumatol 2002;18:281-4.
4. Chosack A, Eidelman E. Rehabilitation of a fractured incisor using the patient’s natural crown-case report. J Dent Child 1964;71:19-21.
5. Simonsen R. Restoration of a fractured central incisor using original tooth fragment. J Am Dent Assoc 1982;105(4):646-8.
6. Olsburg S, Jacoby T, Kreja I. Crown fractures in the permanent dentition: pulpal and restorative considerations. Dental Traumatol 2002;18:103-15.
7. Andreasen JO, Andreasen FM. Textbook and color atlas of traumatic injuries to the teeth. Munksgaard; Copenhagen: 1993.
8. Murchinson DF, Burke FJT, Worthing RB. Incisal edge reattachment: indications for use and clinical technique. Br Dent J 1999;186(12):614-9.
9. Bateman G, Ricketts DNJ, Saunders JP. Fiber-based post systems: A review. Br Dent J 2003;195:43–8.
10. Hornbrook DS, Hastings JH. Use of bondable reinforcement fibre for post and core build up in an endodontically treated tooth: maximizing strength and aesthetics. Pract Periodontics Aesthet Dent 1995;7:33–42.
11. Wadhwani CPK. A single visit multidisciplinary approach to the management of traumatic tooth crown fracture. Br Dent J 2000;11:(188)593-8.
12. Pasini S, Bardellini E, Keller E, Conti G, Flocchini P, Majorana A. Surgical removal and immediate reattachment of coronal fragment embedded in lip. Dental traumatol 2006;22(3):165-8.
13. Shetty PP, Pandya M, Trivedi P, Patel S. Re-attachment: A Conservative Aesthetic Emergency Protocol. Int J Contemp Dent 2011;2(4):113-6.
14. Ricketts DNJ, Tait CME, Higgins AJ. Post and core systems, refinements to tooth preparation and cementation. Br Dent J 2005;198:533–41.
15. Bateman G, Ricketts DNJ, Saunders JP. Fiber-based post systems: a review. Br Dent J 2003;195:43–8.
16. Lanza A, Aversa R, Rengo S, Apicella D, Apicella A. 3D FEA of cemented steel, glass and carbon posts in a maxillary incisor. Dent Mater 2005;21:709–15.
17. Ferrari M, Vichi A, Mannocci F, Mason PN. Retrospective study of the clinical performance of fiber posts. Am J Dent 2000;13:9B–13B.
18. Kavitha T, Rao CVN, Narayan L. Reattachment of fractured tooth fragments using a custom fabricated dowel- Three case reports. Endodontology 2000;12:65-70.
19. Oz IA, Haytaç MC, Toroglu MS. Multidisciplinary approach to the rehabilitation of crown-root fracture with original fragment for immediate esthetics: a case report with 4-year follow-up.Dent Traumatol2006;22(1):48-52.
20. Shetty PP,Metgud S,Jain A,Dhillon G.A conservative single visitreattachment of fracturedcrown fragment.Clinics and Practice 2012; volume 2:e70.p 175-7.
|