INTRODUCTION
Mobile phones are being used in all aspects of health care delivery. They are the much preferred and most used routes of communication. However one aspect that has not been covered is the bacterial contamination of mobile phones.
They are particularly susceptible to this as they are in close contact with mouth, nose, ears, hands and various clinical environments. Futher keeping the mobile phones in pockets, handbags and snug pouches increases the possibility of bacterial proliferation due to warmth and ideal temperature conditions. Mobile phones are continuously used
all day long but never cleaned. Further there are no guidelines for proper disinfection and decontamination of mobile phones thus mobile phones act as resevoirs of infection which may proliferate from patient to patient in a hospital
setting.
First it was hand washing, then it was cleaning of floors and walls,now it has come to light that disease producing bacteria colonize on the dentist ‘s mobile phones Cell phones are being increasingly used for communication as they inexpensive, small and very handy during emergencies. As early as 1861 Semmelweis demonstrated that bacteria were transmitted to patients by hands of health care workers. Mobile phones of dental professionals harbour harmful pathogens and cause severe nosocomial infections. Thus etiological agents of nosocomial infections have found a unique ,significant and perfect way to spread in dental care facilities .
Mobile phones are an important part of dental care and patient management as is the airorter, scaler, etc. While the latter are disinfected, the cell phones are not even cleaned and thus they act as reservoirs and transporters of bacteria from one clinic to another and from one patient to another .
 |
 |
Emergencies in day to day dental practice are excessive and in a hurry the dental professional takes up an emergenicy call without proper hand hygiene being maintained .This becomes even more significant as even the smallest dental
examination involves contact with saliva; and gingival fluid, nasal and mouth breath all potential disease producer as all are in close proximity with the mobile phone. Furthur the aerosol produced by the airoter and scalar are a mixture of saliva and blood which can transmit bacteria over a considerable distance and these bacteria get harboured in nasal and ear cavities and then get transferred to the mobile phone. Due to this aerosol the mere presence of mobile phone in
clinic, can lodge bacteria in them and get transferred with the dental professional moving from one clinic to the other. So this study was to investigate the rate of bacterial contamination of mobile phones of dental professional working in
a teriary dental care facility where dental teaching and complete dental care and treatment is being provided .
MATERIALS AND METHODS
The study was conducted over for a period of six months from Jan 2009 to May 2009 at Himachal Dental College and Hospital, Sundernager H.P
The control group consisted of 200 attendants of patients in O.P.D’s not working in any health care setting and continuously using the mobile phone for atleast fifteen days and who consented for sample collection without prior intimation. . The test group included 200 dental professionals working in various areas of the hospital. These included 110 dental doctor’s (Senior Consultants ,Junior Consultants , Demonstrators ,House Surgeons , Interns ) 60
Dental Paramedics (Dental Technicians, Dental Hygienist, Dental Chairside Assistants, Dental Xray Technicians). 30 other hospital staff (Nurses , Safaikaramchari ) Hospital area wise distributition of test sample included 148 from clinics (Oral Diagnosis , Oral Surgery , Periodontics, Paedodontics , Orthodondics ,Operative Dentistry , Prosthodontics , Oral Radiology ) , 5 from Wards (Oral Surgery), 20 from Special Surgeries (Oral Surgery , Periodontics, Paedodontics , ,Operative Dentistry), 3 from central sterilization room, 24 from post graduate clinics , (Periodontics, Peadodontics , Orthodondics ,Prothodontics ).
SAMPLE COLLECTION
A sterile cotton swab moistened with demineralized water was rolled over all the exposed outer surfaces of the cell phones which were being used for at least 15 days. Care was taken to make sure that all the buttons of the
keypad , mouth piece, earpiece were properly swabbed since these areas are the most frequently in contact with the fingers.
TRANSPORTATION & INOCULATION OF THE SAMPLE
These swabs were transported in sterile tubes containing Cary-Blair transport medium. Later subcultures were made in 5% sheep blood agar, Eosin Methylene –Blue agar and Sabouraud Dextrose Agar.(Hi Media India) Plates were incubated aerobically at 370 C for 24 -48 hours or bacteriological investigation and at room temperature for two weeks for mycological investigation . Isolated microorganisms were identified using gram stain, colony count, and morphology.
Bacteria were identified according to standard protocol (Mackie and McCartney). Test for identification of gram+ cocci included catalase , Oxidative/Fermentative test, anaerobic mannitol fermentation and coagulase production. A slide
coagulase test differentiated stapylococcal isolates into Staphylococcus aureus and coagulasenegative staphylococci (CoNS). Methicillin sensitive staphylococci (MSSA) and Methicillin resistant staphylococci (MRSA) were differenciated by testing with an oxacillin 1 mircogram disk on Muellen –Hinton agar with 4% NaCl and incubated at 350 C for 24 hours as
oxacillin is an analogue of methicillin .
Streptococci were differentiated in to alfa and beta hemolytic groups based upon production of heamolysis on 5% sheep blood agar. For identification of gram negative bacteria a battery of biochemical tests were done. Ceftazidime sensitivity of the gram negative isolates were investigated by disk diffusion method. Swabs were cultured for fungi on
Sabouraud’s dextrose agar and stained with lactophenol cotton blue and further identified by gram staining and KOH wet mounts . Antibiotic sensitivity was done using Kirby –Bauer disc diffusion method on Mueller-Hinton agar.
RESULTS
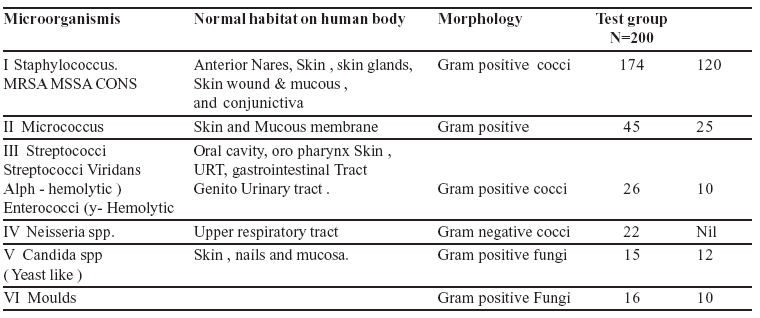
Bacteriological analysis of 200 test Samples revealed that, 189 (94.5%) of them were infected with micro-organisms. Bacteria isolated from mobile phones mainly included; methicillin Sensitive Staphylocouccus, (MSSA), Methicillin
Resistant staphyocuccus aureus, (MRSA) coagulase negative staphylococci,(CONS) micricoccus sp, streptococcus viridans, enterococci spp., Neisseria spp. candida spp; All of these are known to cause nosocomial infection. The number and type of isolates from use of mobile phone of dental professionals of the test group and control group are compared in Table I Further it was found that 54% of mobile phones in the test group were vested with at least
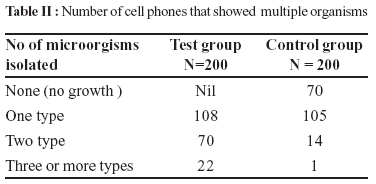
one type of bacteria ; 35% carried two types of bacteria and more than 11% carried three or more group of microorganisms much more than the control group as shown in table II
Table I : Distribution of isolated bacteria from test samples as compared with control groups.
Table II : Number of cell phones that showed multiple organisms
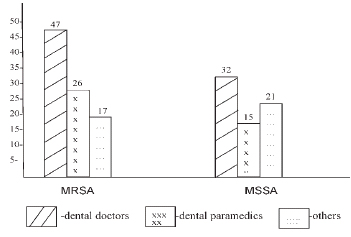
In the control group more number of samples showed one type of microorganism as compared to test group showing that dental professionals have greater potential of bacteriological transfer. Methicillin Resistant staphyocuccus aureus,
(MRSA) was found in 29% of dental professionals
 | Fig 1
|
(MRSA) and methicillin sensitive staphylococcus aureus
(MSSA) Distribution in Dental Professionals
test samples . More worring was that one in every eight handsats showed Methicillin Resistant staphyocuccus aureus, (MRSA) a major virulent strain for nosocomial infections . The control group showed much less presence of MRSA and
MSSA thus less chances of bacterial contamination.
Dental professional wise, these deadly pathogens were found on mobiles phones of 58 dental doctors, 26 Dental paramedices and 17 others (Nurses and SafaiKaramcharis)
Hospital area wise distribution of Methicillin Resistant Staphylococcus Aureus showed.
-
37 Dental professionals working in Operative Dentistry
-
32 Dental professionals working in Periodontics
-
27 Dental professionals working in Oral Surgery and the rest of departments had a nearly equal no. of cases as shown in
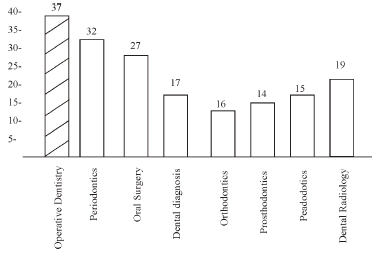 | Fig 2
|
DISCUSSION
This study showed that pathogens which could cause deadly infections were loaded on mobile phones of dental professionals thus indicating that mobile phones of dental professionals were significant vectors on
propagation of cross infection. Further it was found that mobile phones of dental professionals were infected with more than three types of virulent pathogens . One in every eight mobile phone of dental professionals showed the presence of
MRSA. This indicated that mobile phones of dental doctors were more susceptable and bigger transmitter of pathogens,as perhaps they were directly dealing with patients; doing large number of patients ; in direct contact with blood, pus, saliva , and gingival fluid; always working in close proximity with patients, contacting with their
mouth and nasal breath and perhaps keep more than one mobile phone. Hospital area wise distribution of MRSA
showed that dental professionals working in Operative Dentisty, Periodontics, and Oral Surgery were greater transmitter of microorganisms. The reason for this may be that aerosol mixed with blood, pus, saliva and gingival fluids was
produced more in these departments. Pus is known to have larger number of staphylococci. Aerosol of airoters and scalers were potentially hazardous as it could cover greater areas and along with it take harmful pathogens to larger areas of the clinic. Thus the mere presence of mobile phone in the clinic could be potentially significant in the
cross infection.
CLINICAL SIGNIFICANCE & PATHOGENIGTY OF MICROORANISMS FOUND IN THE STUDY
Staphylococcus is present in almost 1/3 of adult human population as asymto matically. Man being the principal; reservoir of staphylococcus which spreads by direct contact or air borne both of which are significant for bacterial transfer from mobile phones. Staphylococcal infection can never be eradicated because of its carrier state in
man. They are normally present in anterior nares, skin, skin gland, mucous membaranes and conjunctiva all in close proximity to mobile phone. Health care workers are known to show higher incidence of carriage of Staphylococcus
Aureus. It causes diseases like boils, Carbuncles, Furuncles , microabcesses. pneumonia, food poisoning, & septicemia especially in diabetic and immuno compromised patients.
Streptococci Veridance, though a normal commensal of mouth, throat and respiratory tract all again in close proximity to mobile phone can cause diseases like bacterial endo carditis, & sepsis. Dental carries is caused by streptococci mutans, Streptococci metor and streptococci sanguis , strains of streptococci.
Entrococci feacalis & enterococci faeciam of enterococcci spp, from human faeces and wounds are documented to cause deadly infection like UTI, infective endocarditis, Billiary tract infection peritonitis, septicemia, & suppurrative
abdominal lesions. Poor hand washing after faecal dischange and wound scratch , leads to in corporation of these bacteria on to hands and nails can subsequently spread by mobile phones, Branhamella a Catarrhalis, a gram negative
cocci of Neissiria spp. are opportunistic pathogen thriving as normal commensals of upper respiratory tract of man are known to cause diseases like otitis media, sinusitis, pneumonia in children and can get transferred from mobile
phones to ears and sinuses of other patients and doctors.
Candidiasis is an opportunistic endogenous infection caused by Candida spp. ,a gram negative fungi. It is the commonest mycosis involving skin and its appendages and mucosa . Mucocutaneous lesions like oral candidiasis , esophageal candidiasis , congunctivitis and keratitis can
spread through mobile phones as fungi and their spores grow well in deep crevices and holes of mobile phones. Skin and nail infection have huge number of candida spp. , which can get transferred to the mobile phones when in contact and subsequently be transferred to other patients.
The warmth of the body, handbags , snugpouches , further potentiates the growth , colonization and proliferation of these virulent pathogens . Food particles from unclean hands provide excellent media for growth of microorgisms as mobile phones are every minute part of our daily life. Sweat from hands and other body parts in a tropical country like ours also acts as excellent medium for transportation and growth of microorgisms .
Similar studies conducted by Brady RRW et al, and Karabay O et al , Indicated that the presence of gram negative bacilli from mobile phones was less ie 4.76%and 7.2% respectively 14,15. Khivsara et al reported 40% contamination
of mobile phones by staphylococcus in health care works in Manglore hospital 16. In another study Karabay et al 2007 reported that E coli, Bacillus Spp, Coagulase negative Staphylococcus which are agents of nosocomial Infections have
been Isolated from mobile phones of healthcare personnel. 20 In Nigeria, Ekrakena and Igeleke (2007) reported that S. Aureus, B. Subtilis, E aerogenes were found in mobile phones of health care staff 19. Studies have reported that objects
like stethoscope, patient files bronchoscope and ball points are vectors for potentially pathogenic microorganisms from health care workers to patients 2,3,4,5, The potential of cell phones as fomites for hospital infection has shown the
presence of Methicilin sensitive Staphylococcus aureus (MSSA), coliforms, methicillin resistant Staphylococcus aureus (MSSA), Corynebacterium spp. Enterococcus faeclais, Clostriduim perfringens, Klebsiella spp, Enterobacter spp,
Pseudomonas spp, Aeromonas spp, Acinetobacter and Stenotrophonmonas maltophilia. 1,12,14, Similarly Brady et al said 14% of mobile phones showed growth of pathogenic bacteria3. In other studies bacterial flora on cell pones showed lower rates of contamination, ranging from 7-14.3% which included MSSA, MRSA, coliforms , Enterococcus faecalis, Clostridium perfringens, Acinetobacter spp, Stenotrophomons maltophila, Pseudomonas spp. and Aeromonas spp 1,8,14,
Comparing these studies with our study a higher percentage (42%) of mobile phones samples were found to be contaminated and 29% of dental professionals had MRSA growing in their mobile phones which we have compared to
MRSA isolates from skin and soft tissue infection of about 18% was significantly higher.
So this study highlights that mobile phones as a potential threat in infection control practices and could exaggerate the role of dental health care associated infection, suggesting that microbial contamination of mobile phones have an
epidemiological risk. Further there are no guidelines for care cleaning and restriction of mobile phones in our dental care settings. It is pointed out that dental professionals should pay special attention to hand hygiene as we believe
that repeated hand washing is the simplest and most economical measure to prevent transfer of harmful pathogens although hand hygiene is greatly over looked and under emphasized in dental care facilities .
The present study did not check the efficacy of various chemical disinfectants for cleaning of mobile phones which needs to be done in future. Further investigations are also required to substantiate the role of mobile phones in transmission of pathogens as this would help to reduce the risk of spread of virulent bacteria from cell phones.
CONCLUSIONS
This study resulted in the following conclusion;
1. 94.5 % mobile phones of dental professionals demonstrated evidence of bacterial contamination with at least one type of bacterial with the potential of causing illness ranging from minor skin rash to deadly disease
.
2. Mobile phones of dental professionals when compared with mobile phones of people not related to medical services were found to have greater potential of pathogen harbour, colinization , proliferation and transfer from
one place to another .
3. Regular and thorough hand washing before and after use of cell phone while doing dental procedures greatly reduces chances of spread of infectious disease .
4. Regular and repeated decontimanation of mobile phones with alcohol containing disinfectant wipes, antibiotic sprays with special attention to mouth piece and keeping mobiles phones in U.V. chambers is are simple methods to reduce bacterial spread.
5. Stress on the use of antimicrobial additive materials for mobile phones is another way to reduce bacterial infection e.g Cellophene lamination of mobile phones reduces crevices where bacteria can harbor as well as makes
mobiles easy to clean.
6. Finally use of cell phones in hospital setting should be strictly limited to emergency calls only as this would greatly reduce cross infection.
7. Lastly creating awareness among dental personnel regarding the role of mobile phones as fomites in transmission of nosocomial infections would go a long way in nosocomial disease preventoin.
REFERENCES
1. Rafferty KM, Pancoast Sj. Bacteriological sampling of telephones and other hospital staff hand-contact objects.J Infect
control. 1984 ;5 (11) :533-5
2. Boyce JM, Opal SM, Chow JW, et al. Outbreak of multidrugresistant Enterococcus faecium with transferable vanB class
vancomycin resistance. J Clin Microbeol. 1984;32;1148-53.
3. Panhotra BR, Saxena AK, Al-Mulhim AS. Contamination of patients’ files in intensive care units: an indication of strict
handwashing after entering case notes. Am J Infect Control.2005;33(7):398-401.
4. Sorin M, Segal-Maurer S, Mariano N, et al. Nosocomial transmission of imipenem-resistant Pseudomonas aeruginosa following bronchoscopy associated with improper connection to the Steris system 1 processor. Infect control. Hosp Epidemiol. 2001;22;409-13.
5. Datz C, Jungwirth A, Dusch H, et al. What’s on a doctors’ ball point pens? Lancet. 1997;350:1824.
6. Wilker PA, Cockerill FR, Craig WA. Performance standards for anti-microbial susceptibility testing:Clinical and lablratory standards institute. 15th informal supplement. 2005. M 100- S15. 25(1).
7. Wayne PA. Khivsara A, Sushma TV, Dhanashree B. Typing of Staphylococcus aureus from mobile phones and clinical
samples. Current science. 2006;90(7):910-12
8. Cathleen M, Braddy MD Janis E, Blair MD. Colonization of personal digital assistants used in a health care setting. American J Infect Control.2005;33:230-2.
9. Dar JA, Thoker MA, Khan JA et al. Molecular epidemiology of clinical and carrier strains of methicillin resistant
staphylococcus aureus (MRSA) in the hospital settings of north India. Ann Clin Microbiol Antimicrob.2006;5:22.
10. Singh D, Kaur H, Gardner WG, Treen LB. Bacterial contamination of hospital pagers. Infect Control Hosp Epidemiol. 2002;23(5):274-6.
11. Pittet D, Boyce JM. Hand hygiene and patient care:Pursuing the Semmelweis legacy. Lancet Infect Dis. 2001;9-20.
12. Brady R.R, Fraser SF, Dunlop MG, Paterson –Brown, Gibb AP. Bacterial contamination of mobile communication devices in the operative environment. J Hosp Infect 2007; 66:397-8.
13. Clinical and Laboratory Standards Institute, Performance standards for antimicrobial disk susceptibility tests; Approved standard, 2005,vol.25,8edn,Mo2-A8th.
14. Brady RR,Wasson A, Stirling I, Mc Allister C,Damani NN. Is your phone bugged? The incidence of bacteria known to cause nosocomial infection on healthcare worker’s mobile phones.J Hosp Infect 2006;62:123-5.
15. Karabay O, Kocoglu E, Tahtaci M. The role of mobile phones in the spread of bacteria associated with nosocomial infectons. J Infect Dveloping countries 2007;1:72-3 . 16. Khivsara A, Sushma T, Dhanashree B. Typing of
Staphylococcus aureus from mobile phones and clinical samples. Curr Sci 2006;90:910-2 .
17. Gupta V, Datta P, Sngla, Skin and soft tissue infection : Frequency of aerobic bacterial isolates and thir antimicrobial
susceptibility pattern. J Assoc Physicians India 2008;56:389- 90.
18. Jaske HC, TiefenthalerW, Hohlrieder Anteking G, Benzer A.Bacterial contamination of anaesthetist’s hands by personal mobile phone and fixed phone use in the operating theatre.Anaesthesia:2007; 62; 904-6.
19. Ekrakene, T. and C.L. Igelake, 2007 .Micro-organisms associated with public mobile phones along bening-sapele
express way, Benin Ciry, Edo State of Nigeria. J.Applied Dci.Res, 3:2009 -2012. |