Introduction
Growth of the craniofacial region is a complex process. It shows variation in rate and direction from infancy to adulthood before leading morphology. Growth prediction has been a controversial topic ever since it was advocated by Ricketts[1]. Prediction would involve forecasting a change in direction or growth rates on the basis of some prior knowledge, such as a cephalometric measurement[2].
Various lateral cephalometric methods have been used to predict the craniofacial growth such as frontal sinus as an indicator of mandibular growth prediction[3], Craniocervical posture, CVMI as a maturity indicator and antegonial notch as a predictor of vertical mandibular growth[4]. The sphenoid sinus is a part of paranasal sinuses and starts developing at 4 months post-conception by constriction of posterosuperior portion of the sphenoethmoid recess and thus passing primary pneumatization. The recess lies in between the sphenoid conchae and the sphenoid body. Secondary pneumatization of the sphenoid sinus occurs at 6 to 7 years in to the sphenoid and basisphenoid bone. Later, the sinus continues to grow up till early adulthood and may invade the wing and rarely the pterygoid plate of the sphenoid bone. Also the sphenoid sinus grows in a downward and forward direction, due to the growth at sphenoccipital suture/synchondrosis.
Therefore, it is hypothesized that the growth of sphenoid sinus may influence the growth of maxillo-mandibular complex. However there is no study correlating the growth of sphenoid sinus with the growth of mandible.
Aim
The aim of the present cross-sectional study is to correlate (using lateral cephalogram) the growth of sphenoid sinus with the mandibular growth.
Material And Methodology
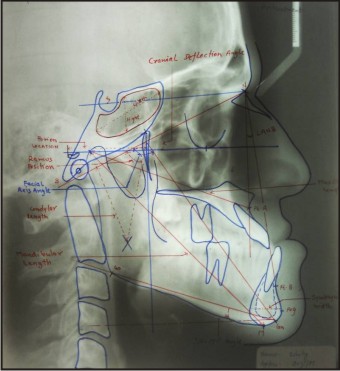
A random selection of 40 cephalograms of adult subjects with skeletal Class I (N=25) or skeletal Class III (N=15) pattern were analysed. The six measurements described by Ricketts were used to determine the presence of abnormal mandibular growth[5]. These were-1.Mandibular length(CO-Gn) 2.Porion location 3.Ramus position 4.Condylar length 5.Symphysis width 6. Cranial Deflection angle.
The size of Sphenoid sinus as expressed in height and width were measured from maximum vertical and horizontal dimension of the sphenoid sinus. The ANB angle was used to ensure that the subjects conformed to skeletal growth difference. The facial axis angle and SN-MP angle were measured to give an indicator of growth direction. Maxillary and mandibular length were measured to give an indicator of the size of bone (Image 1).
Using SPSS 17.0 software, Pearson Correlation Coefficient was used to assess the association between sphenoid sinus height and width with other parameters taken from Lateral Cephalogram. These parameters were Maxillary length,Mandibular length, SN-MP angle ,Facial axis angle, ANB angle ,Porion location,Ramus position, Condylar Length, Symphysis width, Cranial deflection angle.
 | Cephalometric Landmark
 |
Results
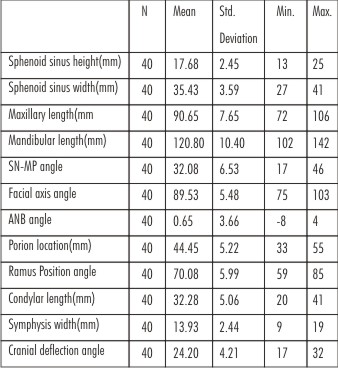
The descriptive statistics of all the variables are given in Table I. The mean sphenoid sinus height and width are 17.68mm and 35.43mm respectively.
The pearson correlation between the sphenoid sinus height and width and other variable maxilla-mandibular growth are given in Table II.
The results show a positive correlation (r=0.507) between sphenoid sinus width and mandibular length which,is highly significant. Also a positive correlation is observed(r=0.440) between sphenoid sinus height and mandibular length which ,is highly significant..
 | Table 1
|
[Image 3]
Other variables that show significant positive correlation with sphenoid sinus height and width are maxillary length(0.424,0,547), porion location(0.552,0.567) and symphysis width(0.466,0.439). However Condylar length(0.354) shows a significant positive correlation with sphenoid sinus width only. Also a Negative but non significant correlation between sphenoid sinus height and ANB angle (r = -0.64) shows a small ANB angle may go with Large sphenoid sinus height .
Discussion
Prediction of abnormal skeletal growth pattern based on morphologic analysis can represent an important step in orthodontic diagnosis and treatment planning. Subjects with mandibular prognathism who can be properly treated by orthodontic tooth movement alone must be distinguished from subjects with mandibular prognathism that require orthognathic surgery.
The size of sphenoid sinus on radiographs is one of the factor that may help the clinician to determine whether he would be able to attain stability by treating a class III malocclusion. For example, with only orthodontic appliances, whether he could expect relapse of the post-treatment results, or whether he should refrain from doing extractions as part of treatment regimen.
A negative ANB angle is indicative of a small maxilla and a large mandible as expressed in the class III syndrome. This is confirmed when the negative correlation for ANB (-0.064) and positive correlation for maxillary(0.424) and mandibular(0.440) lengths are compared with the sphenoid sinus height (Table II).
A long condylar dimension and wide symphysis play a major part in the makeup of a large mandible as seen in Class III subjects. These values show a positive correlation with the large sphenoid sinus size (both height and width).
Thus our study shows that sphenoid sinus can be used as an additional indicator of mandibular growth. The time thus demands a growth of sphenoid sinus with mandibular growth in growing subjects.The guest for use of sphenoid sinus as a skeletal maturity indicator has thus been ignited.
Conclusion
It has been statistically demonstrated in this study that the sphenoid sinus (as seen on the lateral cephalogram) may be a valuable indicator of excessive mandibular growth.Its role in diagnosis shall be a help to the clinician in his attempt to attain excellent treatment results.
References
1. Ricketts RM. Plannig treatment on the basis of the facial pattern and an estimate of its growth. Angle Orthod 1957;27: 14-37.
2. Schulhop RJ, Nakamura S, Williamson WV. Prediction of abnormal growth in class III malocclusions. Am J ORTHOD 1977;71; 421-430.
3. Rossouw P.E and Lombard C.J. The Frontal sinus and mandibular growth prediction Am J Orthod Dentofac Orthop 1991;100: 542-546
4. Odegaard J. Growth of the mandible studied with the aid of a metal implant. Am J Orothod : 1970;57: 145-57.
5. Ricketts RM,Roth RH, Chaconas SJ, Schulhof RJ ,Engel GA. Orthodontic Diagnosis and planning. No.1 Denver, Colorado: Rocky Mountain orthodontics, 1982; 28: 243-260.
6. Ricketts RM. A principal of racial growth of the mandible . Angle Orthod 1972;42:368-386.
7. Dolan KD. Paranasal sinus radiology. Introduction and the sphenoid sinuses. Head and Neck 1982;4: 301-311.
|