Introduction
Esthetics have become increasingly important in the practice of modern dentistry and are synonymous with a natural, harmonious appearance. The term ‘esthetics’ is derived from a greek word meaning perception. It can be divided into two dimensions: objective (admirable) and subjective (enjoyable). Contemporary technique in orthodontics should lend objective esthetics to entire orofacial complex involving form, structure, balance, function and display of dentition[2]. The subject of smile and facial animation as it relates to communication and expression of emotions is of special interest to orthodontists.[3] According to Graber and Salama,[4] an esthetic smile involves relationship between 3 components: teeth, lip framework, and gingival scaffold.
An excessive display of gingiva on smiling, referred to as “gummy smile, “high lip line,” or “high smile line,” is often considered aesthetically displeasing and undesirable.[4],[5],[6],[7],[8],[9] Various etiologic factors including skeletal, gingival, and muscular factors can contribute alone or in combination to this feature.[5],[10],[11] This has led to development of several different modalities for treatment of excessive gingival exposure on smiling that include: surgical crown lengthening/gingivectomy in patients with clinically short anterior tooth crowns,[4] injecting botulinum toxin A to lip elevator muscles in patients with suspected muscular hyperactivity,[11],[12],[13] intrusion with microimplants or orthognathic surgery in patients with vertical maxillary excess.[4],[14]
The purpose of this study was to appraise the upper lip soft-tissue changes in the vertical dimension at both rest and maximum smile, and investigate the correlation between upper labial vestibular attachment height and maxillary gingival exposure on smiling.
Materials And Methods
A total of 54 subjects consisting of 27 males and 27 females volunteered for this study. Exclusion criteria- subjects who had history of: a) Previous orthodontic treatment, b) Maxillofacial surgery, c) Anterior maxillary tooth prosthodontic rehabilitation.
Upper lip position and maxillary incisor crown height at rest and in maximum social smiling were recorded using 9 measurements for each subject. The measurements and the methods used to obtain these variables were as follows:
A) The measurements performed both at rest and maximum smiling :(a) external upper lip length, the vertical measurement from subnasale to stomion superioris (Fig 2-A);(b) vermilion height, the vertical measurement from cupid’s bow to the stomion superioris (Fig 2-B);(c) maxillary central incisor display, the vertical measurement from the stomion superioris to the incisal edge of upper left central incisor (Fig 3-A).
B) The measurements performed once at rest position: (a) internal upper lip length; the vertical measurement, from the labial vestibule apical to the central incisors to the inferior border of the upper lip;(b) maxillary central incisor height, the vertical measurement of the clinical crown height of the maxillary left central incisor (Fig 4).
C) The measurements performed once in maximum smiling when applicable: gingival display in the maximum smiling, the vertical measurement from the inferior border of upper lip to gingival zenith of maxillary central incisor, recorded in patients whose gingival display was noticed in the maximum smile.
All measurements were recorded to the nearest millimetre directly on the face using a simple, small metal ruler. Smile pattern was classified according to the 3 categories described by Tjan et al,[8] relating to the anterior maxillary tooth crown exposure at maximum smile: A) “Low smile” displaying less than 75% of the clinical crown height of the maxillary anterior teeth, B) “Average smile” revealing 75% to 100% of the maxillary anterior crown height, C) “High smile” exposing the whole anterior maxillary crown height and a band of contiguous maxillary gingiva.
 | Fig 1 : Sample Photograph Showing Excessive Ginigival Display
 |
 | Fig 2 (A) External Upper Lip Length, The Vertical Measurement From Subnasale To Stomion Superioris;
|
 | Fig 2 (B) Vermilion Height, The Vertical Measurement From Cupid’s Bow To The Stomion Superioris
|
 | Fig 3 (A) Maxillary Central Incisor Display, The Vertical Measurement From The Stomion Superioris To The Incisal Edge Of Upper Left Central Incisor
|
 | Fig 3 (B) Gingival Display In Maximum Smiling
|
 | Fig 4: Maxillary Central Incisor Height; The Vertical Measurement Of The Clinical Crown Height Of The Maxillary Left Central Incisor
|
Statistical Analysis
Independent Student ‘t’ tests were performed to assess differences between the sexes, and between subjects with and without gingival exposure in maximum smiles. Pearson’s correlation analysis was used to find the relationship between the 2 variables. One-way ‘ANOVA’ was used to assess the differences between smile pattern groups.
Results
Table 1 shows the differences in the measured parameters between females and males. The mean age for the whole study population was 21.85 years with the age range from 19 years to 25 years. The mean age for females was 0.63 years younger than the mean, and the mean age for men was 0.29 years older than the mean. Most of the measured variables showed a statistically significant sexual dimorphism. Relaxed external upper lip length was 2 mm shorter in the women than in the males (P<0.01). The mean maxillary central incisor display at rest was 0.37 mm greater in the females than in males (P<0.005). The upper vermilion comprised 33% of the external upper lip length (34.5% in females and 33.7% in males). Central incisor clinical crown height was 0.28 mm shorter in the females compared with the males (P<.005). External upper lip length became shorter by about 23.6% at maximum smiling in both sexes on an average. High smiles, with exposure of the entire maxillary incisors and a band of gingiva, were noticed in 38.8% of the study population and were 2.9 times more prevalent in females (55.6%) than in males (22.2%). Low smiles, noticed in 51.8% of the subjects, were 2 times more common in males (66.1%) than in females (33.3%). A positive, statistically significant correlation was found between smile patterns and the following: resting external upper lip length, resting maxillary central incisor display, smiling/resting external upper lip length ratio.
 | Table 1: Sex Differences Of Study Parameters
|
Table 2 shows the comparative evaluation of lip measurements in different smile patterns. The mean external upper lip length in subjects with a low smile pattern was 2.47 mm greater than in subjects with a high smile (P <0.05). The mean maxillary central incisor display at rest in subjects with a low smile pattern was 0.86 mm, whereas, in those with a high smile pattern, the mean maxillary central incisor display was 1.66 mm (P<0.05). In the low smile group, external upper lip length in maximum smiling was only 24% shorter than resting external upper lip length; in the average smile group, the external upper lip was shortened by 26%, and in the high group by 50% (P<0.05). Statistically significant differences were found predominantly between between the high and the low smile groups. The findings of this study give more weight to the assumption that patients with a gummy smile have hyper-function of the upper lip.
Although statistically not significant, the resting internal upper lip length/external upper lip length ratio demonstrated a positive correlation between labial vestibule location and smile pattern. In the low smile group, the internal upper lip length was 94.6% of resting external upper lip length; in the average and high smile groups, the internal upper lip lengths were 92% and 90% of the resting external upper lip lengths, respectively.
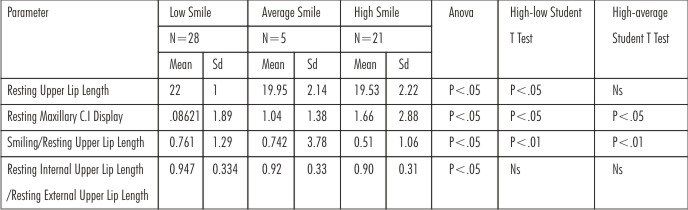 | Table 2: Lip Measurements By Smile Pattern
|
Discussion
Excessive gingival exposure during smiling is considered to be unattractive and is often a challenging issue to many physicians, especially those dealing with smile esthetics.
Data from this study, in concordance with other studies, indicates sexual dimorphism in lip and tooth measurements. These differences reflect simple biologic scaling: male subjects are uniformly larger than equivalent female subjects. Peck et al,[15] who recorded vertical measurements in young orthodontic patients (mean age, 15 years), observed that the difference in upper lip length between the sexes was only 2.2 mm, and that tooth exposure at rest was 5.3 mm in the girls and 4.7 mm in the boys. Hagai Miron et al[16] conducted another study in older orthodontic patients (mean age, 30.5 years) and found a difference in upper lip length of 3.03 mm between the two sexes, but the age-related lip changes reported in the literature do not explain the differences in lengths between the two studies.
In the present study, the upper lip length at rest was found to be 2 mm shorter in the females than in the males. The clinical central incisor crown was 0.28 mm shorter in the females than in the males. The internal upper lip length comprised 92.5% of the external upper lip in females and 94.7% in males. The upper lip length was 25.6% shorter in maximum smiling relative to the resting position in females and 22.2% in males. The findings suggest that a high smile pattern can be considered a female norm, since more than half of the women in this study exposed their gums while smiling, and a low smile pattern can be considered a male norm. Similar results and female/male ratios were observed by others.[8],[13],[15],[16] Ratio of gingival exposure between female and male subjects, was found to be 2.9:1. Although other authors have found a 2:1 ratio of gingival exposure between female and male subjects,[8],[13],[15],[16] in the present study, a slightly higher ratio of 2.9:1 was found between females and males in exposure of gingiva when smiling.
Short upper lip and hyperactivity of the lip elevator muscles are two distinctive features observed in subjects with high smile patterns. In this study subjects with a high smile line had an upper lip on average 2.47 mm shorter than subjects with a low smile pattern.
According to Peck et al,[10] subjects with a gummy smile pattern (more than 2 mm of gingival exposure in maximum smiling) had 20% more muscular capacity to raise the upper lip than did subjects without a gummy smile.
Conclusion
Data from this study indicate sexual dimorphisms in upper lip length, maxillary incisor display, and upper labial vestibule insertion. Higher smile patterns are more common among female patients, and lower smile patterns are more common among male patients. The following findings were observed in subjects with a high smile pattern compared with those with a low smile pattern.
• Short upper lip length.
• Low smiling/resting upper lip length ratio (indicates greater upper lip shortening and might suggest hyperactivity of the lip elevator muscles).
• Low (inferior) attachment of the upper labial vestibule.
References
1. Pilkington EL. Esthetics and optical illusion in dentistry. J Am Dent Assoc; 23:641,1936.
2. Nanda R. Biomechanics and esthetic strategies in clinical orthodontics.
3. Graber, Vanrsdall, Vig. Orthodontics: current principles and techniques.
4. Graber DA, Salama MA. The aesthetic smile: diagnosis and treatment. Periodontol2000;1996:18-28.
5. Ricketts RM. Esthetics, environment, and the law of lip relation. Am J Orthod 1968;54:272-89.
6. Singer RE. A study of the morphologic, treatment, and esthetic aspects of gingival display. Am J Orthod 1974;65:435-6.
7. Janzen EK. A balanced smile—a most important treatment objective. Am J Orthod 1977;72:359-72.
8. Tjan AH, Miller GD, The JG. Some esthetic factors in a smile. J Prosthet Dent 1984;51:24-8.
9. Mack MR. Perspective of facial esthetics in dental treatment planning. J Prosthet Dent 1996;75:169-76.
10. Peck S, Peck L, Kataja M. The gingival smile line. Angle Orthod 1992;62:91-100.
11. Hwang WS, Hur MS, Hu KS, Song WC, Koh KS, Baik HS, et al. Surface anatomy of the lip elevator muscles for the treatment of gummy smile using botulinum toxin. Angle Orthod 2009;79:70-7.
12. Polo M. Botulinum toxin type A in the treatment of excessive gingival display. Am J Orthod Dentofacial Orthop 2005;127:214-8.
13. Polo M. Botulinum toxin type A (Botox) for the neuromuscular correction of excessive gingival display on smiling (gummy smile). Am J Orthod Dentofacial Orthop 2008;133:195-203.
14. Shu R, Huang L, Bai D. Adult Class II Division 1 patient with severe gummy smile treated with temporary anchorage devices. Am J Orthod Dentofacial Orthop 2011;140:97-105.
15. Peck S, Peck L, Kataja M. Some vertical lineaments of lip position. Am J Orthod Dentofacial Orthop 1992;101:519-24.
16. Miron H, Calderon S, Allon D. Upper lip changes and gingival exposure on smiling: Vertical dimension analysis. Am J Orthod Dentofacial Orthop 2012;141:87-93
|