Introduction
Amalgam was taught for decades as the material of choice for restoration in primary molars. Patient demand for better esthetics and parents scare of potential adverse effect of mercury on health and pollution of the environment, motivated manufactures of dental products to develop alternatives for amalgam.[1] With increasing acceptance of adhesive dentistry and the public demand for more esthetics in dentistry, there has been an ever increasing demand by the lay public for tooth-colored restoration, instead of silver or metallic fillings.[2] Aesthetic restorative materials are marketed in various types with different physical characteristics and colors. For direct aesthetic restorations, four types of materials are widely used: composites, compomers, RMGICs and GICs. In pediatric dentistry these esthetically pleasing materials have tremendously changed the concept of today’s practice. These tooth-colored materials are not only used for restoration of decay areas, but are also used for cosmetic improvement of smile by changing the color of teeth and reshaping disfigured teeth.[3] Discoloration is the major esthetic failure of direct tooth-colored restorations. It results from surface staining, marginal staining due to microleakage, changes in surface morphology by wear, and internal material discoloration.
Children with high index of caries usually need a great number of restorations. After the restorative treatment, bacterial plaque control is an important step to prevent secondary caries and pigmentation around margin areas of restoration.[4] Motivation of child patient is a valuable aspect to improve oral hygiene. Dental biofilm is nearly colorless unless stained, so plaque disclosing agents are used to stain the deposits that can be seen distinctly and provide a valuable visual aid in patient instruction.[5] Due to the wide use of tooth-colored restorative materials, it is important to determine which ones are susceptible to color change as the effect of these plaque disclosing agents on the colour stability of restorative materials remains unclear.
Since there is a paucity of information available and in view of limited work done on this aspect, this invitro study was undertaken to compare and evaluate the effect of various plaque disclosing agents on colour stability of various esthetic restorative materials.
Methodology
Thirty six spherical shaped specimens of (compomer (Dyract), Resin- modified glass ionomer cement (Vitremer), Composite resin (Filtek Z350) and Conventional glass ionomer cement (Ketac Fil Plus) each material of dimension of 12 mm in diameter and 1.5 mm in thickness were prepared using brass moulds and the samples were polished with Sof-Lex™ superfine polishing disks. After polishing, the samples were rinsed, dried with paper tissue, and the baseline color measurements were performed. Each Group is then divided into six subgroups (I-VI), each subgroup containing (n=6) six specimens. The six subgroups of each group were exposed to Deionized water (control), Erythrosine based, Bismarck brown based, Basic fuchsin based, Two-Tone and Iodine based disclosing agents respectively for 60 seconds. Then the specimens were rinsed and dried, and final color evaluation was made using spectrophotometer.
Statistical Analysis
The color stability was evaluated by the determination of color change (ΔE*) between the final (F) and the baseline (O) color evaluations, using CIE L*a*b measuring system. The mean values (ΔE*) were calculated for each subgroup pre and post exposure to disclosing agents and analyzed using Students Paired-t-test and inter-comparison between disclosing agents and materials was done using One-Way-Anova with Scheff Multiple comparison test procedure.
The level of significance for all the tests was chosen as p < 0.05.
Results
The result showed that the Compomer (Dyract) and Composite (Filtek Z350), showed significant color change with all the disclosing agents except for control i.e. Deionized water, where as RMGIC showed insignificant color change in Deionized water, Erythrosine and Iodine disclosing agent subgroups and rest all subgroups showed (p<0.05) statistically significant color change and GIC showed statistically insignificant color change in Deionized water subgroup, Two-tone and Iodine based disclosing agent subgroups, where as the remaining subgroups showed (p<0.05) statistically significant color change.
Discussion
Today it is well established that dental plaque is harmful to both teeth and periodontium. Since self cleaning does not occur in modern diet and the use of antiseptic or antibiotics, because of their limitations, have not been introduced in routine plaque control, dental plaque must be removed by other methods, if inflammatory periodontal disease and caries are to be prevented. Effective plaque control must also be the most important part of any dental treatment plan and maintenance care program. Mechanical cleansing procedures are still considered to be the most reliable means of controlling plaque that is not readily visible to the necked eye. As recognition of the (in situ) plaque is considered to be a key factor in patient motivation, the need for disclosing agent arose, and as early as 1914 Skinner introduced the first disclosing agent in the dental literature.During the last twenty years, many investigatorshave suggested that the use of disclosing agents at home is important in patient motivation.[6] Despite the quality improvement of restorative materials, pediatric dentistry treatment reaches a better prognosis when the dental plaque control is done. The oral hygiene motivation should be made several times during the treatment. The plaque disclosing agents improve the motivation of the children. Several plaque disclosing agents have been used: Iodine solution, Mercurochrome solutions, Erythrosine, Basic Fuchsin and organic dye solutions.[4]
Tooth-colored restorative materials provide better esthetic results. Nevertheless, the color stability of tooth-color materials remains a major problem. The color changes can be related to intrinsic changes, such as changes in filler, matrix or silane coating, or extrinsic factors, such as adsorption or absorption of soft drinks, juices, coffee, tea or the products used in dentist’s office. The extent of discoloration in the oral cavity may be associated with dietary habits.[7] Thus one of the side effect of the plaque disclosing agents could be the color change of the tooth-colored restorations. Color changes in esthetic restorative materials have been attributed to a wide variety of possible causes. Many color changes were described as the result of physical adsorption or physico-chemical reactions of the ingredients of the composite material during exposure to the oral environment. Wear or chemical degradation can increase the susceptibility of the material to extrinsic staining. Discoloration of polymeric materials could be due to an oxidation of the un-reacted carbon-carbon double bonds, producing colored peroxide compounds. Other causative factors that may contribute to the change in color of esthetic restorative materials include stain accumulation, dehydration, water sorption, leakage, poor bonding and surface roughness.[8]
In assessing chromatic differences, generally two color systems are utilized, Munsell Color System and Standard Commission International de L’Eclairage (CIELab). In the present study CIE Lab color system was used to evaluate color stability because this color system can transform spectrophotometer data to an approximately uniform color space. In the color space L* indicates lightness, a* indicates (red-green) and b* indicates (yellow-blue) are the chromatically coordinates which indicate color directions.[9] This study investigated the effect of some of the plaque disclosing agents on the surface staining of a range of esthetic restorative materials. Among resin based composite materials (viz compomer, composite and RMGIC), all disclosing agents stained these esthetic restorative materials. Compomer (Dyract) showed highest ΔE values with Basic Fuchsin, and higher ΔE values with Bismarck Brown and Iodine based disclosing agents and was more susceptible to staining than RMGIC (Vitremer) and composite (Filtek Z350).
In the present study compomer (Dyract) showed maximum discoloration when exposed to disclosing agents used in the study (Table-I). There may be number of factors involved in the staining process of compomers, the main reason may be the material may absorb the liquid in the way that it absorbs water,surface reactivity and incomplete polymerization also may have contributed to the color instability of compomers.[7] Compomer absorbs water faster than composite; their hygroscopic expansion is high.[7] Water sorption occurs mainly as direct absorption in the resin matrix. The glass filler particles will not absorb water into the bulk of the material, but can absorb water on to the surface. Thus the amount of water sorption is dependent on the resin content of the material and the quality of the bond between the resin and the filler. Extra water sorption may decrease the life of resin composites by expanding and plasticizing the resin component, hydrolyzing the silane and causing micro-cracks or the interfacial gaps at the interface between filler and matrix allowing stain penetration and discoloration.[10]
 | TABLE I : Comparison Of Pre And Post Color Stability Scores Of Compomer With Different Disclosing Agents.
 |
The composite (Filtek Z350) showed highest ΔE values (Table-III) after exposing to Bismarck Brown based disclosing agent followed by Basic Fuchsin based disclosing agents and also showed significant color change with all the other agents except for the Deionized water (control). Three types of composite material discolorations are generally described (Vermeersch and Vreven 1989); 1) external discolorations due to the accumulation of plaque and surface stains; 2) surface and sub-surface color alterations implying a superficial degradation or a slight penetration and reaction of staining agents within the superficial layer of resin composites (adsorption); or 3) body or intrinsic discolorations due to physico-chemical reactions in the deeper portions of the restorations.[11] Staining susceptibility of resin composites might be attributed to their degree of water sorption and hydrophilicity of the matrix resin. If the resin composite can absorb water, then it is also able to absorb other fluids, which result in discoloration. In the present study all the resin based materials namely composite (Filtek Z350), compomer (Dyract) and RMGIC (Vitremer) showed significant color change with Bismarck Brown based disclosing agent which contains the ethanol and it may be correlated to the higher resin content in these three materials. The color change seen in glass ionomers was minimum, but it was statistically significant.[9]
Bismarck Brown based disclosing agent contained ethanol which may contribute to deterioration of esthetic restorative materials, including some effect on the color stability. Dental polymers have been shown to be susceptible to softening by organic acids produced in plaque as well as ethanol solutions. Since the softening phenomenon is associated with a loosening of polymer structure, an increased propensity to surface staining might be another result of softening. There are many reports[12] in the literature stating that the alcohol in mouth rinses may soften resin based composites restorations, but the mechanism of breakdown is not fully understood. Alcohol is thought to produce stress crazing and cause corrosive effects on the surface of polymeric materials.[9] The color of composite resins may change after exposure to various energy sources and immersion in water for long period.[7]
Although glass-ionomers and poly acid modified resin based composites (Compomers) have a beneficial effects of fluoride release on human dentition, these poly-acid based restorative materials should be used judiciously as substitute esthetic materials for resin based composites in clinical applications.[9] The glass-ionomers produced maximum discoloration with Basic Fuchsin and Bismarck Brown disclosing agents but the extent of discoloration was not very high when compared to the other materials, possible reason may be the glass filler particles will not absorb water into the bulk of the material, but discoloration can be caused by absorption of disclosing solution on to the surface as it absorbs water on to its surface.[10] It has been found that color change of chemically cured materials is associated with the type and quantity of amine involved in the polymerization. Further, the inhibitor has been found to play the role. Besides amine and inhibitor, it has been conjectured that the monomer content and the peroxide may influence internal discoloration.
Since GICs and RMGICs have different compositions, they will not be equally susceptible to surface staining. The results of this study indicated that RMGIC (Vitremer) was more susceptible to staining (Table-II) than Conventional GIC (Ketac Fil Plus) (Table-IV). Previous studieshave shown that the water sorption of Resin-modified glass-ionomers is higher than that of conventional glass-ionomer cements because of the rapid water sorption by HEMA, a significant resin component and accelerated acid-base reaction, but discoloration decreases with time. Fruits et al proposed that Resin-modified glass-ionomers may be chemically stable after sufficient maturation has taken place.[9] Knobloch et al, stated that all Resin-modified glass-ionomer cements showed high water sorption due to their hydrophilic nature. The results of present study confirmed previous findings. Another reason could be related to GICs water content, which is higher in conventional GICs than in RMGICs, such that the former absorbs less water and therefore less susceptible to staining. Glass-ionomers and poly acid modified resin based composites (compomers) may be more adequate for children than adults because in children the materials are less likely to be subjected to long term exposure to organic acids, ethanol, or bleaching agents.
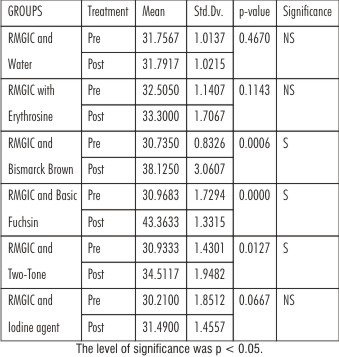 | TABLE II : Comparison Of Pre And Post Color Stability Scores Of Rmgic With Different Disclosing Agents.
|
 | TABLE III : Comparison Of Pre And Post Color Stability Scores Of Composite With Different Disclosing Agents.
|
 | TABLE IV : Comparison Of Pre And Post Color Stability Scores Of Gic With Different Disclosing Agents.
|
Erythrosine is one of the eleven kinds of synthetic dyestuffs permitted to be used in Japan, and it has the largest adsorption index among other dyes. In disclosing agent containing erythrosine showed lesser discoloration of restorative materials, possible reason may be sorption of water might have taken place faster than staining.[13] In the present study, the plaque disclosing agent was applied only one time on the samples. During the treatment, the child can be subjected to several contacts with the disclosing agents. Moreover, there is the action of other kind of products (soft drinks, tea and juices) that could increase the color changes of the restorations.[4]
Combinations of staining solution, immersion time and absence of sufficient cleaning or brushing the specimens during the study are significant factors affecting susceptibility to staining of the materials. However, actual staining in the oral cavity would very likely require longer period of time, because of intermittent nature of stain exposure, because saliva and other fluids will dilute staining media and because restorations will be polished by tooth brushing.
This encouraging invitro data suggests the need for a well controlled clinical trial to evaluate further clinical effectiveness. The verdict of the cumulative experience is awaited.
What This Paper Adds...?
• With increasing acceptance of adhesive dentistry and the public demand for more esthetics in Pediatric Dentistry, there has been an ever increasing demand by the lay public for tooth-colored restoration and it is important to know most color stable material of wide variety of tooth colored materials available in market.
• GIC (Ketac Fil Plus) was the most color stable material which is one of the most widely used cement in Pediatric Dentistry followed by RMGIC (Vitremer), composite (Filtek Z350) and Compomer (Dyract) was the least color stable.
• Erythrosine based disclosing agent (Plaksee) produced least color change among different materials. Bismarck brown based disclosing agent caused maximum discoloration in all tooth colored materials.
References
1. Guelmann M, Mjor I A, Jerell G R. The teaching of class I and II restoration in primary molars: A survey of North American Dental Schools. Pediatr Dent 2001;23:410-4.
2. Stephen H Y Wei. Clinical update of aesthetic dentistry for the 21st century. Dentsply Jan 2000. Hong Kong.
3. Bowel R L, dental filling materials comprising vinyl-silane finished with instruments and materials. J Prosthet Dent 1983;50:351-7.
4. Hino DM, Mendes FM, de Figueiredo JL, Gomide KL, Imparato JC. Effects of plaque disclosing agents on esthetic restorative materials used in pediatric dentistry. J Clin Pediatr Dent 2005;29:143-6.
5. Wilkins EM. Clinical practice of the dental hygienist, 9th ed. Lippincott Williams & Wilkins. 2005; pp383-6.
6. Kipioti A, Tsamis A, Mitsis F. Disclosing agents in plaque control. Evaluation of their role during periodontal treatment. Clin Prev Dent 1984;6:9-13.
7. Abu-Bakr N, Han L, Okamoto A, Iwaku M. Color stability of compomer after immersion in various media. J Esthet Dent 2000;12:258-63.
8. Sarac D, Sarac YS, Kulunk S, Ural C, Kulunk T. The effect of polishing techniques on the surface roughness and color change of composite resins. J Prosthet Dent 2006;96:33-40.
9. Lim BS, Moon HJ, Baek KW, Hahn SH, Kim CW. Color stability of glass-ionomers and polyacid-modified resin-based composites in various environmental solutions. Am J Dent 2001;14:241-6.
10. Bagheri R, Burrow MF, Tyas M. Influence of food simulating solutions and surface finish on susceptibility to staining of aesthetic restorative materials. J Dent 2005;33:389-8.
11. Dietschi D, Campanile G, Holz J, Meyer JM. Comparison of the color stability of ten new-generation composites: An in vitro study. Dent Mater 1994;10:343-62.
12. Ferracane JL, Marker VA. Solvent degradation and reduced fracture toughness in aged composites. J Dent Res 1992;71:13-9.
13. Satou N, Khan A.M, mastsumae I, Satou J, Shintani H. in vitro color change of composite based resins. Dent mater 1989;5:384-7.
|