Introduction
The word provisional means pending a permanent one. Fixed prosthodontic treatment, whether involving complete or partial coverage and natural tooth or dental implant abutments, commonly relies on indirect fabrication of definitive prosthesis in the dental laboratory[1]. Provisional restorations should be the same as definitive restorations in all aspects, except for the material from which they are fabricated[2]. Biologically acceptable fixed prosthodontic treatment demands that prepared teeth be protected and stabilized with provisional restorations that resemble the form and function of the planned definitive treatment[3].
Different materials and techniques have been employed in the fabrication of provisional restoration. The materials may range from acrylic to metals. An ideal material should be easy to handle, have high strength and good tissue compatibility[4].
This study aimed to evaluate the flexural strength of three different provisional restorative materials under conditions that simulate the stresses acting on them to those acting on a fixed partial denture and determine clinical application of the results.
Materials And Methodology
This study was conducted at Department of Prosthodontics and Crown & Bridge, Genesis Institute of Dental Sciences and Research, Ferozepur and Central Institute of plastic and Engineering Technology, Murthal to evaluate flexural strength of provisional restoration fabricated using different materials. The materials used for testing were Heat cure Polymethylmethacrylate resin (Dental Products of India, Mumbai), Autopolymerising Polymethyl metacrylate resin (Dental Products of India, Mumbai) and Protemp-4, Bisphenol-A-glycidil Methacrylate-4 (3M ESPE Deutschland, Germany).
A total of 90 samples were fabricated and divided into three groups. Each group consisted of 30 samples divided according to type of materials:
Group A: Autopolymerising resin
Group B: Pro temp 4
Group C: Heat cure resin
The method used in the study was divided into the following steps -
1. Fabrication of precision die:
Two abutments second premolar and second molar on the left lower quadrant of typodont set were selected, simulating as lower left quadrant of patient with missing first molar. The trough that was created after removing the first molar was filled by modelling wax to represent a residual edentulous space. Ideal tooth preparation was done with a chamfer finish line and uniform taper of 60 (approximately). After tooth preparation perforated sectional metal stock tray was selected for making the impression. Tray adhesive was applied and polyvinyl siloxane putty and light body impression material (3M ESPE AG, Seefeld Germany) was used for making impression. Impression was scraped for creating space for light body. After setting of material sectional tray was removed and impression was inspected. Molten blue inlay wax was poured into the impression for fabrication of wax pattern. After solidification of wax pattern it was retrieved, sprues were attached at an angle of 450 (approximately) on the non functional cusp. Cobalt chromium alloy was used for casting. All procedures of investing, casting, finishing and polishing were done to get a precision die. The exposed root portion of both the abutment and residual edentulous space was covered by autopolymerising resin block (Figure 1a).
 | Fig 1 (a) : Precision die
 |
2. Fabrication of all metal fixed partial denture:
Wax pattern for three unit fixed partial denture using second premolar and second molar as abutment was fabricated on precision die. A bar sanitary pontic design was selected for the fabrication of wax pattern by using inlay wax. After making of wax pattern, it was checked for any defect. Sprues were attached at an angle of 450 (approximately)on the non functional cusp. Cobalt chromium alloy was used for casting the F.P.D in metal. Elective induction and standard procedure was used to obtain error free casting. Three unit F.P.D was checked that it should seat properly over the precision die without any rocking and had self retention with good marginal fit (Figure 1b).
 | Fig 1 (b) : All metal F.P.D
|
3. Construction of custom tray:
An index of precision die along with all metal fixed partial denture was made using Polyvinyl siloxane putty and light body impression material (3M ESPE AG, Seefeld Germany). The index was poured with dental stone, two sheets of modelling wax were adapted and sealed over the stone model. All standard procedures of flasking, dewaxing, packing and curing with heat cure acrylic resin (Dental Products of India, Mumbai) were carried out according to manufacturer instruction. A handle was prepared using self cure resin (Dental Products of India, Mumbai). Sufficient Perforations in tray were made with number 8 round bur.
4. Making of master impression :
Block out of dead space below the three unit F.P.D on precision die was done with putty. Tray adhesive was applied to custom tray, Polyvinyl siloxane putty and light body impression material (3M ESPE AG, Seefeld Germany) was used to yield a master impression which was used for construction of interim prosthesis samples (Figure 2).
 | Fig 2 : Master impression
|
5. Fabrication of autopolymerising resin samples (Group A) :
Tooth coloured polymethyl methacrylate (PMMA) acrylic resin (DPI Dental Products of India Ltd, Mumbai, India) was used to make the interim prosthesis samples. The samples were fabricated with the polymer to monomer ratio as per manufacturers recommended ratio of 3:1 by volume. Resin mixture was poured into the master impression which was then placed on the metal die. The sample was retrieved from the master impression and the excess was trimmed and sample was finished and polished. Ten such samples were prepared in one impression. Though there were negligible chances of distortion, but to rule out any change in the samples three impressions were made for accuracy and safety. Thirty such samples were prepared and were subjected to three point bending test using universal testing machine.
6. Fabrication of Protemp-4 samples (Group B):
Protemp 4 is a composite materials for fabrication of provisional restoration. Material was loaded in master impression, using a new mixing tip each time. A small amount of material was extruded from mixing tip on to mixing pad and discarded then the material was injected into the master impression and then placed over the metal die. According to manufacturer instructions material attained a hard elastic consistency within 1 min 40 sec. The master impression was removed from the metal die within 2 min 50 sec. Sample was retrieved. The oxygen inhibitor layer was removed using alcohol. Sample was then finished using fine carbide burs. Thirty such samples were prepared and were subjected to three point bending test using universal testing machine.
7. Fabrication of Heat cure resin samples (Group C):
Polymethylmetacrylate heat cure resin (Dental Products of India, Mumbai) was used for the fabrication of provisional restoration. First of all impression with Polyvinyl siloxane putty and light body impression (3M ESPE AG, Seefeld Germany) was made of metal die and poured in dental stone. Molten wax was poured into the master impression and placed over the metal die for fabricating wax pattern. After solidification of wax, pattern was retrieved and sealed over stone model of metal die. Flasking, dewaxing and processing was done following according the standard protocol and manufacturer instructions for this material. Samples were finished and polished Thirty such samples were prepared and were subjected to three point bending test using universal testing machine.
8. Measurement of flexural strength of samples:
Metal die was fitted within the jaws of fixture. Each sample fitted snugly on the die (Figure 3). The test samples were loaded with a 1.5 mm diameter of stainless steel pin placed in the specifically demarcated region of the sample, i.e. the central fossa of the pontic with a crosshead speed of 5 mm/min till the fracture occurred (Figure 4). The load resulting in fracture of the sample was recorded using the software attached to universal testing machine.
Flexural strength was automatically calculated by the equipment software (the reading displayed on the system) using the formula: FS = 3 W L/2 b d2, where
FS = flexural strength (MPa or MN/m2), W = maximum load before fracture (N ), L = distance between the supports (mm), b = width of the samples (mm) and d = thickness of the samples (mm). All the collected data was subjected to statistical analysis.
 | Fig 3 : Precision die with sample fitted in fixture and load application on central fossa of pontic
|
 | Fig 4 : Fractured sample
|
Results
The samples were subjected to three point bending test under Universal Testing Machine (Instron) and the values were obtained. The results were subjected to statistical analysis by applying one – way ANOVA (Analysis of Variance) and Post Hoc Tukey HSD tests (for multiple comparisons) and graphs were plotted.
The mean value of flexural strength was highest for Group C (Heat cure resin) i.e. 563.1137, followed by Group B (Pro temp 4) i.e. 523.7173 and Group A (Autopolymerising resin) i.e. 323.2993 (Table 1 and Graph 1).
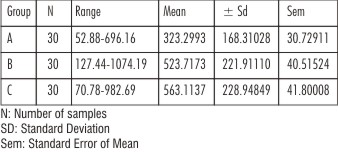 | Table 1 : Flexural Strength (Mean ± Sd) Values
|
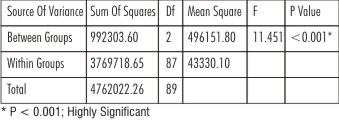 | Table 2 : One Way Anova (Analysis Of Variance)
|
By applying Oneway Analysis of Variance, a statistically significant difference in flexural load was seen within groups and between groups i.e. p < 0.001 (Table 2).
Post Hoc Tukey HSD tests were applied to make multiple comparisons between different groups. At 0.05 level, statistically significant mean difference values were seen between the following groups – A & B, A & C and B & C. p value < 0.05 was obtained between Groups A & B which is statistically significant. p value < 0.001 was obtained between Groups A & C which is statistically highly significant. p value > 0.05 was obtained between Groups B & C which is statistically not significant.
The provisional restorations fabricated using heat cure resin showed the highest mean flexural load of 563.1137 N followed by Protemp 4 (523.7173 N) and self cure resin (323.2993N).
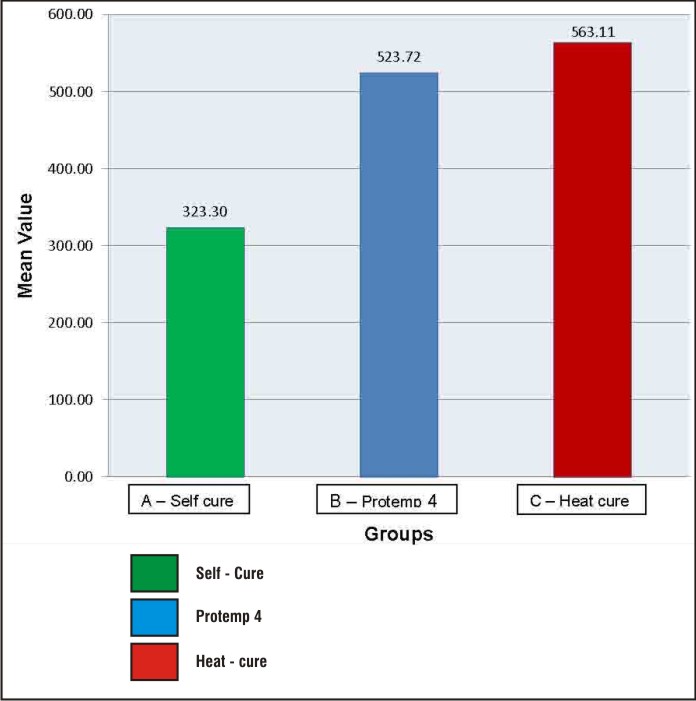 | Graph 1 : Mean Flexural Strength In Different Groups
|
Discussion
Interim restorations are an essential part of fixed prosthodontic treatment. Patients must be provided with an interim restoration from initial tooth preparation until the definitive prosthesis is placed.
Unsatisfactory strength of self cure resin results in failure or partial breakage of provisional FPDs over time. Traditional PMMA resin provisional FPDs typically fracture owing to heavy occlusal stress. This results in clinical inconvenience due to the need to rehabilitate or replace the FPDs, which is much more difficult for the dentist. The frequent mechanical failures of provisional fixed prostheses usually cause inconvenience, loss of time, and embarrassment for both dental clinicians and patients and also loss of confidence for dental clinicians before definitive restoration.
For patients with bruxism or those whose treatment plans require long term use of provisional restorations, when periodontally involved teeth to be retained during osseointegration of an implant, provisional restoration with improved physical properties are required. Temporomandibular joint observations demands prolonged use of provisional fixed partial denture. Therefore it is imperative to fabricate provisional fixed partial denture in sufficiently strong materials to avoid frustrating moments for clinician and patient.
Flexural Strengthis the stress that is necessary to cause fracture or a specified amount of plastic deformation. One method to evaluate the ability to withstand the functional loads is to evaluate the material’s flexural strength, also known as transverse strength, which is the strength of a material under a static load. This measurement is a combination of tensile and compressive strength tests with elements of proportional limit and elastic measurements[5]. According to the International Organization for Standardization (ISO 4049) and the American National Standards Institute (ANSI) / American Dental Association (ADA) Specifications # 27, an interim fixed prosthesis material must have a minimum strength of 50 Mega Pascals (MPa) when a bar of the material undergoes a 3-point bend test.
Interim fixed dental prosthesis are subjected to flexure under function and the fracture can occur under occlusal load resulting in failure of the restoration. Therefore, the interim restorations should have adequate flexural strength to withstand the masticatory forces. Although, restorations should be properly designed to avoid it, they may nevertheless fail leading to discomfort and time loss. The flexural strength of interim restoration materials is one of the important factors and should be considered prior to selecting a provisional restorative material for the clinical success.
Studies have been carried out to modify the chain structure for enhancing the flexural strength of materials. Protemp 4 is a Bis acrylic resin composite material, in which the manufacturer modified the chain structure of Bis acrylic resin composite materials to increase the flexural strength. Bis acrylic resin composite materials are difunctional and capable of cross linking with another monomer chain. This cross-linking imparts strength and toughness to the material. Protemp 4 is based on these modifications in which instead of rigid intermediate chain characteristics of some Bis-acrylic homologues, it also has flexible chain in comparison to other synthetic resin.
S. Dagar et al. 2005conducted a study on direct and indirect provisional materials and found that Protemp 2 has lesser flexural strength as compared to heat cure polymethyl methacrylate but more than self cure poly methyl methacrylate[4]. Singhal Romil et al 2012 conducted a study for flexural strength of four different provisional restorative materials. It was concluded that highest mean flexural strength was Heat cured acrylic resin followed by auto polymerized composite resin (Protemp-3), auto polymerized cold cured acrylic resin and light cured composite resin[6].
In the present study, three chemically different, commercially available crown and bridge provisional restorative materials were chosen to test and compare the flexural strength. Group (A) Autopolymerising resin, Polymethyl metacrylate (Dental Products of India, Mumbai), Group (B) Protemp-4, Bisphenol-A-glycidil Methacrylate-4 (3M ESPE Deutschland, Germany), Group (C) Heat cure resin, Polymethylmethacrylate(Dental Products of India, Mumbai). The materials we have chosen were based on their popular use, chemical composition differences and recent advances. Various advantages of PMMA are ease of availability, cost effective, easy to finish and polish and can be repaired easily.
In the study mean flexural strength was highest for Heat cured acrylic (563.11 N) followed by Protemp 4 (523.72 N) and least for Self cured acrylic (323.30 N). PMMA resins are relatively inexpensive, with good color stability, excellent polishability, and good marginal adaptation. Though materials have some draw backs like exothermic reaction, polymerisation shrinkage, low strength and pulpal irritation associated with excess free monomer but their ease of fabrication, cost effectiveness and good marginal adaptability outweigh their draw backs.
Visible light-cured urethane dimetha crylates have controllable working time, good wear resistance, low temperature changes, and good color stability. Their disadvantages include poor marginal fit, brittle nature, and high cost. Selection of a material should be based upon consideration of all the properties of the material in addition to its flexural strength and hardness. In spite of following a standard protocol for preparing, curing, and finishing of the test specimens, the homogeneity of mix, presence of internal porosity, pressure, and the release of stresses during finishing and polishing procedures was not controlled.
In the oral cavity, the provisional restoration is exposed to forces of varying magnitudes acting in different directions, and there are also temperature variations. The same situation was not simulated in this in vitro study. No correlation between effects of varying span length and different types of food solvents on the mechanical properties of the provisional restorations was done. Therefore further investigations are required under more closely simulated clinical conditions.
Conclusion
Based on the observation of present study it is recommended that in posterior long span fixed partial denture and in full mouth rehabilitation cases, the material of choice should be heat polymerizing PMMA or protemp 4 because of increased demand on strength of material to tolerate functional stresses. In anterior region Protemp 4 is recommended to be used because magnitude of functional stresses is comparatively less than posterior region. In certain surgical cases where an immediate provisional restoration is required Protemp 4 is material of choice because of ease of manipulation of direct fabrication. In addition it has advantage of no exothermic reaction and compatibility with eugenol temporary cement. Self cure acrylic resin may be put in to limited use of single provisional crown.
References
1. Luthardt RG, Stossel M, Hinz M, Vollandt, R. Clinical performance and periodontal outcome of temporary crowns and fixed partial dentures: a randomized clinical trial. J Prosthet Dent 2000;83:32-9.
2. Higginbottom, FL. Quality provisional restorations: a must for successful restorative dentistry. Compend Contin Educ Dent 1995;16:442-444-7.
3. Fox CW, Abrams BL, Doukoudakis A. Provisional restorations for altered occlusions. J Prosthet Dent 1984;52:567-72.
4. Dagar S, Pakhan A, Tunkiwala. An in-vitro evaluation of flexural strength of direct and indirect provisionalization materials. J Indian Prosthod Soc 2005;5:132-35.
5. Anusavice KJ. Phillips’ science of dental materials. 10thed Philadelphia: WB Saunders; 1996. p. 237-71.
6. Singhal RA, Kumar S, Agarwal S et al. An Evaluation Of Flexural Strength Of Different Provisional Restorative Materials- An In-Vitro Study. Indian Journal of Dental Sciences 2012;4:17-19.
|