|
|
|
| Comparative Evaluation Of Antimicrobial Activity Of Different Herbal Extracts And 2% Chlorhexidine Gluconate Against E. Faecalis & C. Albicans: An In Vitro Study. |
Anuradha Rani 1 , Savita Thakur 2 , Shavina Gupta 3 , Preeti Gauniyal 4 , Marisha Bhandari 5 , Hitesh Gupta 6
1 Professor & Head , Dept. of Conservative Dentistry & Endodontics - HIDS, Paonta Sahib
2 PG Student , Dept. Of Conservative Dentistry & Endodontics - HIDS, Paonta Sahib
3 Senior Lecturer , Dept. of Conservative Dentistry & endodontics - HIDS,Paonta Sahib
4 Senior Lecturer , Dept. of Microbiology - HIDS, Paonta Sahib
5 Senior Lecturer , Dept. of Conservative Dentistry & Endodontics - HIDS, Paonta Sahib
6 Reader , Dept. of Conservative Dentistry & Endodontics - HIDS, Paonta Sahib
|
| Address For Correspondence |
Dr. Sohinderjit Singh
Professor & Head
Dept. Of Orthodontics
Himachal Institute of Dental Sciences, Paonta Sahib |
| Abstract |
| AIM
To compare anti-microbial efficacy of herbal extracts with that of 2 % Chlorhexidine against Enterococcus faecalis and Candida albicans.
Material and Methods
The antimicrobial activity was determined using agar diffusion test. Samples were divided into 4 groups : Group A 2% Chlorhexidine Gluconate (positive control), Group B – 5% garlic extract, Group C- 5% turmeric extract Group and Group D– Distilled water (negative control ). The zones of inhibition of growth were recorded.
Statistical Analysis Used
Statistical analysis was performed using One way Anova with post-Hoc Turkey’s HSD and was statistically significant (P < 0.05).
Result
Maximum inhibitory effect against Enterococcus faecalis was shown by Chlorhexidine followed by turmeric and then garlic. Maximum antimicrobial activity against Candida albicans was shown by garlic followed by Chlorhexidine and then turmeric. Conclusion Herbal extracts showed significant inhibitory effects against Enterococcus faecalis and Candida albicans which are comparable with 2% Chlorhexidine. |
|
| Keywords |
| Herbal Extracts, Candida Albicans, Enterococcus Faecalis, Chlorhexidine |
|
| Full Text |
Introduction
The role of microorganisms and their byproducts in the initiation and perpetuation of pulpal and periapical pathology has been well established. The main objective of endodontic treatment is the elimination of infected pulp tissue and microorganisms from the root canal system and prevention of subsequent re-infection to achieve complete peri-radicular healing.[1]
It is generally believed that the major cause of post-treatment disease after root canal treatment is the persistence of microorganisms in the apical part of the root canal of root filled teeth.[2] Enterococcus faecalis and Candida albicans are the most commonly isolated species in persistent root canal infections.[3]
Enterococcus faecalisaccounts for up to 22 to 77% of therapeutic failures because of its inherent ability to tolerate starvation and extreme pH (upto11.5), salt concentration, bio-film formation, dentin tubular invasion and emergence of antibiotic resistance.[4]
Candida albicanshas been isolated in persistent root canal infections is 2.9 to 22.2 % of cases. Its ability to form biofilm by adhering to the dental tissues utilizing its hyphae to penetrate into the dentinal tubule as well as secretion of proteases and hydrolytic enzymes add to its pathogenicity.[5]
Complete debridement and adequate elimination of microbial irritants is a fundamental prerequisite for successful endodontic therapy. Among the procedures involved in the control of endodontic infection, irrigation is an important step in eliminating micro-organisms from the root canal system. An ideal root canal irrigant should have potent anti-microbial activity, ability to dissolve remaining pulp tissues as well as should be non-toxic and non-carcinogenic. It should be relatively inexpensive, easily available and convenient to apply.[6]
Chlorhexidine Gluconate, a cationic bis-guanide is a broad spectrum antimicrobial agent and is effective bactericidal and fungicidal agent. It has been used as an irrigant and intracanal medicament in endodontics in concentration of 2 %.[7] A major advantage of Chlorhexidine is its substantively, which allows prolonged residual antimicrobial effect.
2% Chlorhexidine solution is irritating to the skin and have toxic effect on host tissue if expressed beyond the confines of root canal. In addition, its cytotoxic effects on human osteoblasts might indicate its ability to impair the regenerative potential of the periapical tissues and can thus impairs healing.[8]
The constant increase in antibiotic resistant strains and side effects caused by synthetic drugs has prompted researchers to look for herbal alternatives. The importance of this problem has been emphasized in WHO World Health Day theme for the year 2011 “COMBAT ANTIBIOTIC RESITANCE”.[9]
With time plant extracts have been understood to encompass the attributes accounted not only for their fragrance and flavor but also for their antimicrobial nature. Various natural plant extracts have known antimicrobial and therapeutic effects suggesting their potential to be used as an endodontic irrigant. Phytochemical extracts such as Curcuma longa (turmeric) and Allium sativum (garlic) consists of active ingredients like Curcumin and Allicin respectively which have anti microbial, anti inflammatory and anti-oxidant properties.[10],[11]
The efficacy of these herbal extracts has been evaluated in the present study for their antimicrobial activity against Enterococcus faecalis and Candida albicans (the most resistant endodontic pathogens) to assess their possible future use as root canal irrigant/medicament.
Materials and Methods
In the present study, the aqueous extracts of Garlic and turmeric were taken as the experimental groups for their antimicrobial effect, whereas 2% Chlorhexidine Gluconate was taken as positive control and distilled water as negative control. Enterococcus faecalis (MTCC 439) and Candida albicans (MTCC 854) strains were used in this study to check antimicrobial activity.
Groups were divided as under:
Group A- 2% Chlorhexidine Gluconate (Positive control)
Group B – 5% Garlic extract (Experimental group)
Group C- 5% Turmeric extract (Experimental group)
Group D- Distilled water (negative control)
Preparation of extracts: Whole plants of garlic and turmeric were procured from botanical Gardens of Himachal Institute of Dental Sciences (HIDS), Paonta Sahib (H.P) and were cleaned using distilled water. Fresh peeled cloves of garlic and rhizomes of turmeric were shade dried and powdered in a mechanical grinder. 5 grams each of air-dried garlic and turmeric powder were macerated with 100 ml of distilled water. The homogenate of garlic and turmeric powder was filtered using Whatman’s filter paper no. 1. These extracts of garlic and turmeric were heated over water bath for 5-6 hrs till they become viscous. The anti- microbial tests was started on the same after preparation of extracts.
Preparation of cultures: Pure strains of Enterococcus faecalis (MTCC 439) and Candida albicans (MTCC 854) were obtained from the Department of Microbiology, HIDS, Paonta sahib (H.P). Pure culture of E.faecalis and C.albicans was added to two test tubes containing 10 ml peptone water and Sabouraud Dextrose Broth respectively. The test tubes were incubated at 370C for 24 hrs. Cultures were adjusted to a 0.5% turbidity reading on McFarland scale.
Agar diffusion method: Hundred Micro-liters each of E.faecalis and C.albicans suspensions were taken from prepared cultures and inoculated in 130 mm culture plates with previously set layers of Mueller Hinton and Sabouraud Dextrose Agar respectively (Hi Media Labs). Inoculations were performed by using sterile spreader across media. Uniform wells of 7 mm diameter and about 2 centimeter apart from each other were made in each culture plate with the help of sterile cork-borer (Fig 1). About 100 µl of herbal extracts (garlic and turmeric) were added using sterilized micropipette into the prepared wells. 100 µl each of 2% Chlorhexidine Gluconate (positive control) and distilled water (negative control) were also added into other wells for control. The plates were incubated at 37°C for 24 hours for Enterococcus faecalis and 37°C for 48 hours for Candida albicans. All the procedures were done under strict aseptic conditions using laminar air flow chamber. The diameters of bacterial inhibition zones were recorded in millimeters around each well.
Results
The mean values of growth inhibition in mm recorded for 2% Chlorhexidine, Turmeric (5%) and Garlic (5%) against E.faecalis are given in Table 1 and Graph-1 and the culture plates showing zones of inhibition are shown in Figure 1.
 | Table 1 (Mean Zone Of Inhibition – Enterococcus Faecalis)
 |
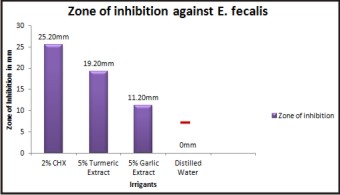 | Graph 1
|
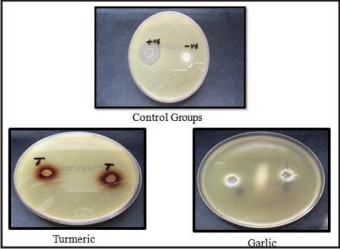 | Fig 1 - Culture Plates Showing Zones Of Inhibition Against Enterococcus Faecalis
|
The Graph1 depicts that mean zone of inhibition was highest for Chlorhexidine (25.3) > Turmeric (19.2) > Garlic (11.2) > Distilled water (00). From the results of One Way ANOVA, the mean zone of inhibition of five groups were statistically significant from each other at F=1549.279, P=<.001.
The mean values of growth inhibition produced by 2% Chlorhexidine, Turmeric (5%), Garlic (5%) against C.albicans are given in Table 2 and Graph 2 and the culture plates showing zones of inhibition are shown in Figure 2.
The Graph 2 depicts that mean zone of inhibition was highest for Garlic (32.2) > Chlorhexidine > Turmeric (18.9) > Distilled water (00). From the results of One Way ANOVA, the mean zone of inhibition of five groups were statistically significant from each other at F= 3363.750 P= <.001.
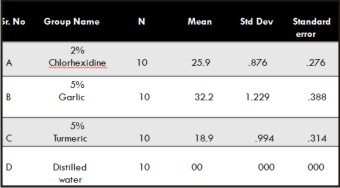 | Table 2 (Mean Zone Of Inhibition – Candida Albicans)
|
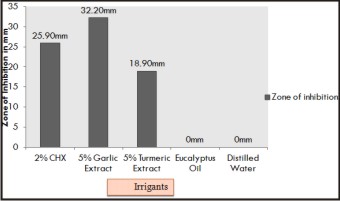 | Graph 2
|
 | Fig 2 - Culture Plates Showing Zones Of Inhibition Against Candida Albicans
|
Discussion
The main objective of root canal therapy is the elimination of microorganisms from the root canal system and the prevention of recontamination after treatment. The complex anatomy of the root canal system limits the mechanical action of endodontic instruments. Chemical debridement by endodontic irrigant solutions are used to facilitate the debridement and disinfection of the root canal space. Thus, mechanical enlargement of canals must be accompanied by copious irrigation in order to facilitate maximum removal of micro-organisms.[12]
Despite the antimicrobial properties of the irrigants, elimination of microorganisms may not be uniform because of the varying vulnerabilities of the involved organisms. Primary endodontic infections are polymicrobial, typically dominated by obligatory anaerobic bacteria. The most frequently isolated microorganisms before root canal treatment include Gram-negative anaerobic rods, Gram-positive anaerobic cocci, Gram-positive anaerobic and facultative rods, Lactobacillus species, and Gram positive Streptococcus species. The obligate anaerobes are rather easily eradicated during root canal treatment. On the other hand, facultative bacteria such as Staphylococcus, Enterococci, once established, are more likely to survive chemo-mechanical instrumentation and root canal medication.[13]
In particular Enterococcus faecalis has gained attention in the endodontic literature, as it can frequently be isolated from root canals in cases of failed root canal treatments. In addition, yeasts may also be found in root canals associated with therapy resistant apical cases and chronic apical periodontitis as they are more resistant to antimicrobial agents usually used in endodontics.[12]
Chlorhexidine gluconate (CHX) is widely used in disinfection because of its excellent antimicrobial activity. It has potent and substantive antimicrobial activity against some resistant bacteria such as Enterococcus faecalis and fungi Candida albicans.[14]
In our study, the zone of inhibition with 2% CHX was bigger than herbal extracts (5% Turmeric and 5% Garlic) for E.faecalis. Its efficacy is because of the interaction of the positive charge of the molecule with the negatively charged phosphate groups on microbial cell walls which alters the cells osmotic equilibrium. This increases the permeability of the cell wall, allowing the CHX molecule to penetrate into the bacteria. Damage to this delicate membrane is followed by leakage of intracellular constituents, particularly phosphate entities such as adenosine triphosphate and nucleic acids.
This finding is in agreement with a study carried out by Kandaswamy, Eswar et al where 2% CHX showed the maximum efficacy against E.faecalis as compared to garlic and calcium hydroxide.[15]
This is not in agreement with another study by Hemanshi Kumar, where 20% turmeric (Curcuma longa) showed larger zone of microbial inhibition than CHX gel 1%.[16] The difference may be due to more concentration of turmeric and lesser concentration of CHX used in the present study.
In the present study, 5 % garlic (Allium sativum) extract showed maximum antifungal efficacy whereas activity against E.faecalis was mild as compared to CHX and turmeric. Garlic contains at least 33 sulphur compounds, several enzymes, 17 amino acids, and minerals such as selenium. It contains a higher concentration of sulphur compounds than any other Allium species. The sulphur compounds are responsible both for garlic’s pungent odour and many of its medicinal effects. Dried, powdered garlic contains approximately 1% Allicin (S-allyl cysteine sulfoxide). One of the most biologically active compounds, allinin (diallyl thiosulfinate or diallyl disulfide) does not exist in garlic until it is crushed or cut; injury to the garlic bulb activates the enzyme allinase, which metabolizes allilin to allicin. Allicin is further metabolized to vinyldithines.
Allicin was assumed to be the main component responsible for the inhibition of fungal growth. A concentrated garlic extract containing 34% allicin, 44% total thiosulfinates, and 20% vinyldithiins possessed potent in vitro fungistatic and fungicidal activity. Allicin inhibits both germination of spores and growth of hyphae. The main antimicrobial effect of allicin is due to its chemical reaction with thiol groups of various enzymes such as e.g. alcohol dehydrogenase, thioredoxin reductase, and RNA polymerase. This could be the possible reason for the antifungal efficacy of garlic extract.[17]
This finding is in agreement with a study carried out by Heon-J in Leea and Hani A. Masaadeh et al according to which garlic extract has maximum efficacy against C.albicans and mild activity against E.faecalis[18],[19]
Turmeric (Curcuma longa) used extensively in foods for both its flavor and color, as well as having a long tradition of use in the Chinese and Ayurvedic systems of medicine, particularly as an anti-inflammatory and for the treatment of flatulence, jaundice, hematuria, hemorrhage, and colic. Turmeric can also be applied topically in poultices to relieve pain and inflammation. Curcumin (diferuloylmethane) the main yellow bioactive component of turmeric has been shown to have a wide spectrum of biological actions, including anti microbial, anti – inflammatory and anti- oxidant activities, anti bacterial and has immune regulatory functions.[10]
In this study, the turmeric has shown good antimicrobial efficacy against E.faecalis and mild activity against C.albicans. This finding is in synchrony with a study done by Thilla S Vinoth Kumar according to which turmeric showed good inhibitory activity against E.faecalis and C.albicans.[13]
A study by Vibha Hegde et al has concluded that turmeric has shown good antimicrobial efficacy only against C.albicans which is contradictory to the results of this study.[20]
Conclusion:
The present in-vitro study explored the potential clinical application of herbal extracts in the root canal by finding the antimicrobial activity against the most resistant microorganisms in persistent root canal infections compared with that of Chlorhexidine.
On the basis of the results obtained in present study, the following can be concluded:
Garlic extract showed the superior anti fungal action against Candida albicans as compared with Chlorhexidine and mild activity against Enterococcus faecalis
Turmeric showed the comparable activity against Enterococcus faecalis and Candida albicans as compared to CHX.
However, further ex-vivo studies followed by clinical studies are recommended to determine the potential use of garlic and turmeric extracts as intracanal irrigant as well as intracanal medicaments during root canal treatment.
References:
1. Neelakantan P, Sanjeev K and Subbaro C.V. Duration-dependent susceptibility of endodontic pathogens to calcium hydroxide and chlorhexidene gel used as intracanal medicament: an in vitro evaluation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;104:e138-e141.
2. Peciuliene V, Maneliene R, Balcikonyte E et al. Microorganisms in root canal infections: a review. Stomatologija, Baltic Dental and Maxillofacial Journal 2008;10(1):4-9.
3. Vinothkumar TS, Rubin MI, Balaji L and Kandaswamy D. In vitro evaluation of five different herbal extracts as an antimicrobial endodontic irrigant using real time quantitative polymerase chain reaction. J Conserv Dent 2013;16(2):167-170.
4. Nair P. N. R. Review on the causes of persistent apical periodontitis: a review. Int End J 2006;39:249–81.
5. Siqueira JF (Jr), Rocas IN, Lopes HP, Elias CN, de Uzeda M: Fungal infection of the radicular dentin. J Endo 2002; 28(11): 770-773.
6. Basrani B & Haapasalo M. Update on Endodontic irrigating solutions. Endodontic Topics 2012; 27: 74–102.
7. Kandaswamy D, Venkateshbabu N ,Gogulnath D and Kindo A.J. Dentinal tubule disinfection with 2% chlorhexidine gel, propolis, morinda citrifolia juice, 2% povidone iodine and calciumhydroxide. Int Endod J 2010;43:419-423.
8. Luddin N, Ahmed H. The antibacterial activity of sodium hypochlorite and chlorhexidine against Enterococcus faecalis: A review on agar diffusion and direct contact methods. J Conserv Dent 2013;16(1):9-16.
9. Giriraju A, Nagesh L, Bajaj S. Evaluation of antimicrobial potential of 10% ginger extract against streptococcus mutans, candida albicans and enterococcus faecalis – an in-vitro study. International Journal of Science Innovations and Discoveries 2012;2(1), 260-265.
10. Neelakantan P, Jagannathan N and Nazar N. Ethnopharmacological approach in Endododontic Treatment: A Focused Review. Int. J. Drug Dev.& Res.,Oct-Dec 2011;3(4):68-77.
11. Dhinahar.S and Lakshmi.T. Role of botanicals as antimicrobial agents in management of dental infections.- review. International Journal of Pharma and Bio Sciences 2011;2(4):B-691-704.
12. Gomes BPFA, Vianna ME, Sena NT et al. In vitro evaluation of antimicrobial activity of calcium hydroxide combined with chlorhexidene gel used as intracanal medicament. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006;102:544-50.
13. L. E. Chavez De Paz, G. Dahlen, A. Molander, A. M¨oller, and G. Bergenholtz, “Bacteria recovered from teeth with apical periodontitis after antimicrobial endodontic treatment,” Int Endod J 2003;36(7):500-508.
14. D Kandaswamy, N Venkateshbabu. Root canal irrigants- a review. J Conser Dent 2010; 13( 4 ): 256-264.
15. Kandaswamy E, Venkateshbabu N, Rajeswari K, Kandaswamy D. Dentinal tubule disinfection with 2% chlorhexidine, garlic extract, and calcium hydroxide against Enterococcus faecalis by using real-time polymerase chain reaction: In vitro study. J Conserv Dent 2013;16(3):194-198.
16. Kumar H. An in vitro evaluation of the antimicrobial efficacy of Curcuma longa, Tachyspermum ammi, chlorhexidine gluconate, and calcium hydroxide on Enterococcus faecalis. J Conserv Dent 2013;16(2):144-147.
17. Ankri S, Mirelman D. A Review: Antimicrobial properties of allicin from garlic. Microbes Infect 1999;2:125-129.
18. Leea HJ, Parkb HS, Kimc KH, Kwond TY and Honge SH. Effect of garlic on bacterial biofilm formation on orthodontic wire.Angle Orthod 2011;81(5):895-900.
19. Masaadeh HA, Hayajneh WA and Momani NM. Microbial Ecology of dental plaques of Jordanian patients and inhibitory effects of Allium sativum and Allium cepa L. extracts. J Med Sci 2006;6(4):650-653
20. Hegde V, Kesaira DP. Comparative evaluation of antimicrobial activity of neem, propolis, turmeric, liquorice and sodium hypochlorite as root canal irrigants against E. Faecalis and C. Albicans - An in vitro study. Endodontology 2013;25(2):38-45.
|
|
|
|
|
|
|