Introduction
Virtual technologies in dentistry will be used to provide better education and training by simulating complex contexts and enhancing procedures that are traditionally limited, such as work with mechanical articulator[1]. Currently, the mechanical articulator is used for the functional simulation of the effects of dysmorphology and dysocclusion. However, this mechanical scenario, so very different from the real life biological setting, poses a series of problems. In effect, the movements reproduced by the mechanical articulator follow the margins of the structures that conform the mechanical joint, which remain invariable over time, and which cannot simulate masticatory movements that are dependent upon the muscle patterns and resilience of the soft tissues and joint disc. Moreover, tooth mobility cannot be simulated by plaster models; as a result, the latter are unable to reproduce the real life dynamic conditions of occlusion[2],[3]. There are also other problems derived from the procedures and materials used for assembling the models in the articulator: precision in orienting the model, expansion and contraction of the plaster, deformation of the bite-recording material, the stability of the articula-tor, etc.[3]. Because of these basic problems, the reproduction of dynamic, excursive contacts seems to lower the reliability. Although they adjusted the articulator with computerized axiographic data, Tamaki et al[4] report that only 82% of the teeth in the mechanical articulator reproduce protrusive contacts and 90% reproduce laterotrusive contacts. 66% of the protrusive and 81% of the laterotrusive contacts was correctly located. The mechanical articulator also creates new contacts[5]. VR is intended to help solve these problems
The virtual articulator offers the possibility of significantly reducing the limitations of mechanical articulators[6], due to a series of advantages: full analysis can be made of static and dynamic occlusion, of the inter-maxillary relationships, and of the joint conditions, thanks to dynamic visualization in three dimensions (3D) of the mandible, the maxilla or both, and to the possibility of selecting section planes allowing detailed observation of regions of interest such as for example the temporo mandibular joint[3]. This tool incorporates virtual reality applications to the world of dental practice with the purpose of replacing mechanical articulators and thereby avoiding the errors and limitations of the latter Combined with CAD/CAM technology, this tool offers great potential in planning dental implants, since it affords greater precision and a lesser duration of treatment[1].
Szentpetery’s virtual articulator: It was introduced by Szentpetery in 1999. It is based on a mathematical simulation of the articulator movements. It is a fully adjustable 3D virtual dental articulator capable of reproducing the movement of an articulator. But as it is a mathematical approach, if behaves as an average value articulator and so not possible to obtain easily the individualized movement paths of each patient[7],[8].
Virtual articulator of Kordass and Gartner: It was introduced by Kordass and Gartner in 2003, based on the exact registration of mandibular movement with the help of jaw movement analyzer. This virtual articulator system requires digital 3D representation of the jaws as input data generates an animation of the jaw movement and delivers a dynamic and tailored visualization of the collision points[2],[9].
Virtual articulator based on mechanical dental articulator: It was introduced by graphic design and engineering project developments, the University of the Basque Country in 2009. It is more simple approach than the virtual articulator developed by Kordass and Gaertner and at the same time more accurate result can be obtained than the Szentpetery’s virtual articulator. The main advantage of this approach is that the user can choose the most suitable articulator to use in the simulation[2].
Programming And Functioning Of Virtual Articulator
The programming and adjustment methods of the virtual articulator were described by Kordass and Gärtner in 1999. First a digital image is obtained of the surfaces of each tooth, of the global dental arches, and of the bite registries. To this effect a three-dimensional laser scanner is used, such as for example the Laser Scan 3D (Willytec, Munich, Germany) [Fig: 1]. This scanner projects a vertical laser beam onto the surface of the object. A digital camera equipped with a charge coupled device (CCD) registers the beam reflected from the object and transmits the digital signals to an electronic processing system. The processed image data are stored as digital matrix brightness values, ready for use by the scanner software and for on-screen visualization and computerized manipulation[10]. In this phase, the real geometry of the mouth and its relation location are reconstructed in a CAD system using face bow[11].
 | Figure 1 : Laser Scan 3d
 |
Selection of the articulator
The selected articulator[12], and even more importantly, the skill and care, with which it is used, have a direct effect/impact on the success of fixed or removable restorations. Since the intercuspation position is static, the articulator will need to act only as a rigid hinge, which is little more than a handle for the model. The mandible, however, does not act as a simple hinge. Rather than this, it is capable of rotating around axes in three planes. The occlusal morphology of any restoration for the mouth must accommodate the free passage of the antagonist teeth without interfering with the movement of the mandible. Because of their potential to produce pathologies, occlusal interferences must not be incorporated into restorations placed by the dentist. One way of preventing this problem is the use of fully adjustable articulators which simulate mandibular movements with a high degree of precision. Treatments using these articulators are time consuming and demand a great skill from both dentist and technician. As a result, the cost of such treatments does not make it feasible for minor routine treatment plans.
Virtual articulator design process
Once the articulators are selected, their structures and shapes are analyzed in order to clarify how to use the Reverse Engineering and measuring tools. The general structure, this is, upper and lower bodies, is similar in both articulators, but the TMJ-s, which are the most important part of the articulators, present a great variety of configurations.
Hanau H2
The Hanau H2 has been modelled using ATOS I 3D scanner , in order to have the drafts located on the correct position in space. To get the sections of the scanned point cloud, the Rapidform XOR software has been used. The whole articulator has been constructed combining both measured and scanned parts. Once the Virtual Articulator is constructed, all the measures are verified. The final step deals with locating the models on the articulator. For this purpose, the relative position of the upper model is scanned using the face bow. Afterwards, the location in the virtual articulator is direct, and the location of the lower model is made using an electronic bite in Centric Relation. Then, the virtual articulator is ready to apply the kinematic simulation using the CATIA CAD system[2],[9].
Stratos 200
The Ivoclar Stratos 200 has been modelled using a SolidEdge CAD system. Some parts were modelled directly after measuring the mechanical dental articulator. However, the Handyscan 3D scanner has been used, due to its mobility, and almost all the articulator has been scanned. Using Geomagic point cloud edition software, the useful data has been taken from the millions of points that had been scanned.Finally, as it has been done with Hanau H2, the models have been located in the correct position, ready to apply the kinematic analysis.
Functioning of the Virtual Articulator
After the articulator is modeled, the simulation is run and any possible interference on the designed prosthesis are checked out and if they are present corrected accordingly[7].
The basic system of the virtual articulator generates an animation of the movements of the mandible based on the input data, and calculates the points of occlusion, which in turn are shown on-screen by means of some type of code [3].
Ideally, the virtual articulator is equipped with a device for registering the specific mandibular movements of a given patient (such as the Jaw Motion Analyser system) [Fig: 2], and can integrate the movements recorded in the animation. This system is based on measuring the velocity of ultrasonic impulses emitted from three transmitters attached to the lower sensor. Four receivers are attached to a face bow opposite them. This positioning enables the detection of all rotative and translative components in all degrees of freedom. A special digitizing sensor is used to determine the reference plane, which is composed of the hinge axis infraorbital plane and special points of interest (eg, on the occlusal surface).
There are also other systems for the detection of mandibular movements based on other technologies, such as optoelectronic devices that use CCD cameras to register the emissions of light-emitting diodes (LEDs) positioned over the head of the patient and generate an image from these signals[13].
If JMA tool is not available for registering the mandibular movements, specific movements must be defined by means of parameters, in a way similar to the practice used with mechanical articulators. Some parameters of interest in these cases would be the following: protrusion (radius of the condylar guide, maximum distance of condylar protrusion), retrusion (radius of the condy-lar guide, maximum distance of retrusion), laterotrusion (maximum protrusion, Bennett angle, radius of the right and left condylar guide, right and left horizontal condylar slope, phase angle, lateral displacement), and aperture / closure slope (maximum angle of aperture). After defining the movement parameters, collision detection is required in order to identify the movement re-strictions. In these cases, it may be of interest to leave a distance corresponding to the thickness of the occlusion paper used in the mechanical articulators, for calculating the points of occlusion on the basis of this distance[3].
 | Figure:2 : Jaw Motion Analyser
|
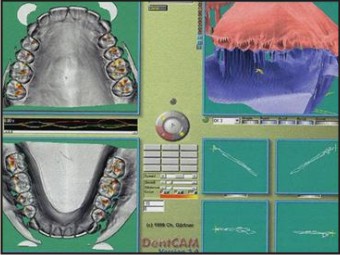
As an example, the software of the Dent-CAM® virtual articulator [Fig: 3] (Comp. KaVo, DLeutkirch) uses three main windows that show the same movement pattern, distinguishing a series of aspects:
 | Figure:3 : Dent-cam Software
|
a) interpretation window: this shows both maxilla in dynamic occlusion and allows us to obtain unusual points of view, e.g., observation from an occlusal surface of closing of the opposing tooth during mastication.
b) occlusion window: this shows the points of contact that appear on the occlusal surfaces of the upper and lower teeth as a function of time.
c) section window: this offers different frontal sections along the dental arch. This tool can be used to analyze the degree of intercuspidation, as well as the height and functional angles of the cuspids.
The latest software versions incorporate an orthodontic module allowing the creation of a virtual setup. The program has also been equipped with the representation of the condylar trajectories in the sagittal and horizontal planes. This tool allows us to observe the inter-relationship between the incisal guide and the condylar guide, and the effects of joint mobility upon occlusion[10].
One of the most recent new developments in the virtual articulators is the 3D virtual articulation system (Zebris company, D-Isny). This system requires the following:
a) an input unit in the form of a 3D scanner
b) the software for prosthesis modeling and collision detection, based on a virtual articulator
c) the output module (a rapid prototyping system). With this system, and in addition to mandibular movement, we can analyze masticatory movement – including force at the points of contact and the frequency of contacts in relation to time[14].
Validation:
The results of validation were recently presented[15],[16]. Comparing the model situation of a mechanical articulator (KaVo, Leutkirch, Germany) to the virtual articulator module, DentCAM showed approximately the same number of dynamic contacts in lateral movements to the left and right in eight cases (mechanical articulator: 90, virtual articulator: 92). The results demonstrate the correspondence under standardized conditions in relation to the detected number of contacts in both situations[17]. To examine reliability, three operators measured the mandibular movements two times in eight persons. After data implementation, data matching, and programming of the VR articulator, good correspondence was demonstrated in visualizing the number and position of dynamic contacts[16]. In this same line, Pröschel et al.[18] carried out a study of 57 asymptomatic patients in order to determine the occlusal errors appearing in the mechanical articulators. To this effect comparisons were made with the virtual articulator, yielding an error in the second molar of 200 μm in 16% of the patients and of 300 μm in 6% of the subjects – this implying a low risk of error, though the acceptable limits in clinical practice could be exceeded. Likewise, other studies have compared the maximum number of contacts between the conventional method and the virtual articulator – the occlusal contacts calculated from the virtual models being shown to precisely reproduce the contacts obtained with the mechanical articulator[19],[20].
Future Work
In future there is a need to develop a virtual articulator software that integrates the correcting software for CAD/CAM system directly into the process of construction of crowns and bridges .
A digital face-bow transfer is not possible. At present, the face bow has to be mounted on the patient and then brought to the dental mechanical articulator. Finally, it is important to remark that several improvements should be made up when obtaining the patient's data. This is a main shortcoming which generates difficulties on the next step, this is, the use of the articulator and the design process. Therefore, a progress in this sense will bring important improvements on the whole process.
Conclusion
The VR articulator is undoubtedly more than an entertaining novelty. The virtual articulator is a precise tool for the full analysis of occlusion in a real patient, and can help the dental professional in establishing a diagnosis and in planning the best treatment option. Another remarkable conclusion is the flexibility and versatility offered by this type of Virtual Articulator. The add-on modules will change conventional ways of production and communication in dentistry and begin to replace the mechanical tools.
Acknowledgements
I would like to express my gratitude to my colleagues at J.S.S Dental college especially Dr Amrutha V.S for their help and support
References
1. Bisler A, Bockholt U, Kordass B, Suchan M, Voss G. The virtual articulator. Int J Comput Dent. 2002;5:101-6.
2. Böröcz Z, Dirksen D, Thomas C, Runte C, Bollmann F, von Bally G. Investigation of influencing variables on the computer-aided simulation of contacts in dynamic occlusion based on optically digitized plaster casts. Biomed Tech (Berl). 2004;49:111-6.
3. Kordass B, Gärtner C, Söhnel A, Bisler A, Voss G, Bockholt U, et al. The virtual articulator in dentistry: concept and development. Dent Clin North Am. 2002;46:493-506
4. Tamaki K, Celar AG, Beyrer S, Aoki H. Reproduction of excursive tooth contact in anarticulator with computerized axiography data. J Prosthet Dent 1997;78:773–9.
5. Gsellmann B, Schmid-Schwap M, Piehslinger E, Slavicek R. Lengths of condylar pathways measured with computerized axiography (CADIAX) and occlusal index in patients and volunteers. J Oral Rehabil. 1998;25:146-52.
6. Hayashi T, Saitoh A, Ishioka K, Miyakawa M. A computerized system for analyzing occlusal relations during mandibular movements. Int J Prosthodont. 1994;7:108-14.
7. Solaberrieta E, Etxaniz O, Minguez R, Muniozguren J, Arias A, editors. Design of a Virtual Articulator for the Simulation and Analysis of Mandibular Movements in Dental CAD/CAM. 2009: Cranfield University Press.
8. Strub JR, Rekow ED, Witkowski S. Computer-aided design and fabrication of dental restorations: Current systems and future possibilities. The Journal of the American Dental Association 2006;137:1289-96.
9. Fasbinder DJ. Clinical performance of chairside CAD/CAM restorations. The Journal of the American Dental Association 2006;137:22S-31S.
10. Gärtner C, Kordass B. The virtual articulator: development and evaluation. Int J Comput Dent. 2003;6:11-24.
11. Hogden J, Lofqvist A, Gracco V, Zlokarnik I, Rubin P, Saltzman E. Accurate recovery of articulator positions from acoustics: New conclusions based on human data. Journal of the Acoustical Society of America1996;100:1819-34.
12. Hobo, S., Herbert, T., Whitsett, D., Articulator Selection for Restorative Dentistry. Journal Prosthetics Dentistry. 1976,
13. Fang JJ, Kuo TH. Modelling of mandibular movement. Comput Biol Med. 2008;38:1152-62.
14. Ruge S, Kordass B. 3D-VAS--initial results from computerized visualization of dynamic occlusion. Int J Comput Dent. 2008;11:9-16.
15. Kordaß B, Ga¨rtner CH. Virtual articulator: usage of virtual reality tools in the dental technology. Quintessence of Dent Tech 2000;12:75–80.
16. Ga¨rtner CH, Kordaß B, Gesch D, et al. Virtueller Artikulator DentCAM 3.0 Okklusionsanalyse fu¨r Funktionsdiagnostik und Kieferorthopa¨die zur Reproduzierbarkeit der Befunde. Zahnaizteiche Welt Rewur .2000;11:607–12.
17. Kordaß B, Ga¨rtner CH. Matching von digitalisierten Kaufla¨chen und okklusalen Bewegungsaufzeichnungen. Dtsch Zahnarztl Z 1999;5:399–402.
18. Pröschel PA, Maul T, Morneburg T. Predicted incidence of excursive occlusal errors in com-mon modes of articulator adjustment. Int J Prosthodont. 2000;13:303-10.
19. Delong R, Ko CC, Anderson GC, Hodges JS, Douglas WH. Comparing maximum intercuspal contacts of virtual dental patients and mounted dental casts. J Prosthet Dent. 2002;88:622-30.
20. Maruyama T, Nakamura Y, Hayashi T, Kato K. Computer-aided determination of occlusal contact points for dental 3-D CAD. Med Biol Eng Comput. 2006;44:445-50.
|