Soft linings are compliant, viscoelastic materials used to form all or part of the fit surface of a denture. Their complete function is debatable, but they serve to distribute the forces of mastication more evenly and to absorb energy.Soft lining materials can be defined as soft, resilient, elastic materials which form a cushioned layer between the hard denture base and the oral mucosa. They are broadly divided in to two groups of materials. The first group includes the tissue conditioners and temporary soft lining materials typically based on polyethyl methacrylate, an aromatic ester and ethyl alcohol. The second group includes the permanent soft lining materials based on silicone rubber or acrylic resin.[5]
History
The earliest soft lining material “velum” was used by Twitchell in 1869. However this material had high water absorption and it became foul smelling and ill fitting after a period of time.[2]
In 1945 Matthews[2] used poly (vinyl chloride) powder with a liquid di-n-butyl phthalate plasticizer in the form of a paste as a facial prosthetic material and soft lining for patients with chronic mucosal tenderness.
Lammie and Storer[2] described the use of poly (vinyl chloride) plasticized with di-buty[1] phthalate and found it to be a very unsatisfactory material because of it’s high water absorption,hardening and cracking.
In the late 1940s Nelson[2] used butyl phthalate, butyl glycollate as a plasticizer for vinyl chloracetate because he believed that this plasticizer improved the adhesion b/w the lining and the poly (methyl methacrylate) denture base.
Wichterle and Lim[2] in 1961 used “softdent” softlining material but it changed its volume when immersed in water. Later in 1958 silicone rubber materials based on poly (dimethyl siloxane) have been used as soft lining material.
Currently Available Materials:
During last 20 yearsavailable materials can be divided into 5 groups.
• Heat polymerized acrylic resin.
• Auto polymerized acrylic resin.
• Heat polymerized silicones.
• Auto polymerized silicones.
• Treatment liners (Tissue conditioners)
Both heat processed and Auto polymerizing acrylic resign soft lining material consist of powder and liquid components[20]
Composition of 2 acrylic resin soft lining materials
Vertex soft
• Powder----poly (ethyl methacrylate)
• Monomer----acetyl tributyl citrate+ methyl methacrylate Coe soft–
• Powder-- poly (ethyl methacrylate)
• Monomer--Di-n-butyl phthalate + benzyl salicylate + ethyl alcohol
The chemical composition of acrylic resin soft lining is similar to that of the acrylic resin denture base material thus no adhesive is required to form bond.
Composition of two silicone soft lining material
Molloplast
Polymer-polydimethyl siloxane
Monomer - Acryloxy alkyl silane,Benzoyl peroxide
Flexibase
Polymer-polydimethyl siloxane
Monomer-Triethoxysilanol,Dibutyl tin dilurate
Adhesive-methacryloxy propyl trimethoxysilane
The silicone liners remain soft for extended periods of time. However in some patients it has been observed that a yeast Candida albicans- may grow within the liner, resulting in a rough and hardened surface. Inhibitors have been proposed to eliminate this problem. These do not adhere as well to denture bases as plasticized acrylic resin does. Some silicone liners also have poor tear resistance, particularly after storage in water for extended period[21].
Ideal properties
For maximum efficiency soft lining materials should display the following properties;
1. They should be easily processed using conventional laboratory equipment.
2. They should exhibit minimal dimensional change during processing and such change should be the same as that of the denture base materials.[3]
3. Water absorption should be minimal[4]. Ideally, the total water absorption should be close to that of the acrylic resin denture base polymers, reported as 2.2%.[14].
4. The materials should have minimal solubility in saliva[4].
5. They should retain their resiliency. The degree of resilience will depend on the chemical composition of the material and the thickness of soft lining. Several authors[7],[13],[14] suggest that a thickness of 2-3mm is most appropriate.
6. They should bond sufficiently well to poly (methylmethacrylate) to avoid separation during use which may lead to difficulty in cleaning.[1]
7. Adequate tear resistance.
8. They should be easily cleaned and not affected by food, drink or tobacco. It is also important that the resilience and surface texture of the lining be unaffected by freely available denture cleansers of all types.
9. They should be nontoxic,odourless and tasteless to encourage long term wear of the denture by the patient.
10. They should be aesthetically acceptable and their color should match that of the denture base material.
Limitations of use
The use of soft lining material on the fit (impression) surface of the denture is limited by a number of factors. These include:
Reduction of the denture base strength:
When inter ridge distance is limited and the denture base thickness is minimal, the placement of a soft lining will further reduce the overall strength of the denture and inevitably increase the tendency of the denture base to fracture.
1. Loss of softness and resilience:
Some of the soft linings are not stable in an aqueous environment such as the oral cavity. This is true of those materials using a plasticizer to increase softness or resiliency. Since the plasticizer will leach out and cause the lining to harden and limit its usefulness. Thermal effects from the ingestion of hot and cold food and drinks may also have a deleterious effect.
1. Colonization by Candida albicans:
It has been suggested that the porosity of soft linings allows water absorption and the diffusion of nutrient material, which can easily become colonized by Candida organisms.
1. Difficulty in keeping soft linings clean using the normal denture cleaning methods: The use of conventional denture cleansers may cause bleaching and the surface may become bubbled if an oxygenating cleaner is used.[2]
2. Dimensional instability:
Some soft lining loses their plasticizer with time and most of them absorb water.[3],[5],[14],These factors may cause dimensional changes.
1. Failure of adhesion:
A common problem of soft lined dentures is the failure of adhesion between the soft lining and the denture base. This can be predicted from laboratory studies.[1]
1. Difficulties in finishing and polishing.
Difficult to trim, finish and polish. If excessive force is used, they may overheat or tear ,leading to poor surface finish.
Clinical uses:
1. Ridge Atrophy or Resorption
2. Knife edged mandibular ridges
3. useful in areas where bone and skin grafts are used to improve the edentulous ridges
4. used for the cleft palate patient, or an acquired oral defect related to trauma, to improve the retention of the denture by engaging the undercuts.
5. Salivary gland disturbances or degenerative changes result in a reduced salivary flow-which can result in loose dentures as well as discomfort and soreness—a soft lining may be indicated to reduce load transmission and so limit the effect of poor lubrication.
6. Hyperemic and traumatized oral mucosa often associated with ill fitting poorly occluding dentures
7. Patients with avitaminosis.
8. Temporary obturators
9. Stabilizers of base plate and surgical splints or stents
10. Adjunct in the impression making procedure or as a final impression material
11. Restoration of congenital and acquired oral defects
12. Post irradiation- to prevent excessive irritation.
13. Systemic and local factors causing tissue soreness
 | Manipulation
 |
Laboratory Technique For Acrylic Soft Liners
Preparation:
Prepare the denture base for the soft liner by relieving the acrylic tissue-bearing surface by 2mm or more. .Eliminate severe undercuts.Gently scrub the upper half of the flask (denture half) and rinse with hot water. Apply separator to stone or plaster.
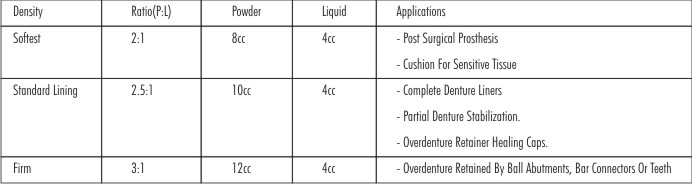
Measuring & Mixing: take the measured quantity of powder and liquid in mixing cup; Stir very slowly until all of the powder particles are totally moistened. The mixture instantly turns “sticky”and “honey-like.”consistency
Curing:
In a flask: Place flask in a curing unit filled with boiling water (212°F/100°C) for 15 minutes.
In a jig: Place jig in a curing unit or in a pressure pot at (20psi/1.4bar) in steaming hot water (between 125°F/50°C to165°F/74°C) for 10 minutes.
Finishing:
Remove cured denture from flask or jig; chill it a few minutes in an ice water bath to temporarily harden the soft liner for easy trimming. Remove excess flash with sharp scissors, scalpel or suitable rotary instrument (i.e. acrylic bur, rubber point or finishing stone). If desired, finish with a wet rag wheel and pumice to further smooth the surface. Do not high-shine the liner using a buff wheel.
Sealing: Dry the liner surface using air blower to remove all surface moisture. Apply a generous coat of Sealer over the totally dry soft liner and air dry for more than 2 minutes. Repeat procedure adding a second coating. A third coat of Sealer can be applied on non-retentive fitting surfaces.
Chair Side Technique
Preparation: Prepare the denture base for the soft liner by relieving the acrylic tissue-bearing surface by 2mm or more. .Eliminate severe undercuts Clean and dry the areas where the soft liner is to be applied. Use petroleum jelly or a water soluble substitute to coat the interproximal surfaces that are not meant to be lined. This will ease finishing.
Measuring & Mixing: same like laboratory technique.
Curing: Place the denture in steaming hot water (between 125°F/50°C to 165°F/74°C)and cure for 10 min using pressure pot.
Finishing & Sealing: Same like laboratory technique
Patient Delivery: Give patient a Patient Care Card to instruct him/her on care and cleaning of the soft liner. Soak only 10 min. in denture cleaner. Warn patient not to scrub the soft liner with a hard - bristle brush; andRequest annual re-sealing of soft liner and dental examination to assure proper fit.
Disinfection: Silicone Elastomers are affected by the metabolites produced by Candida albicans and other microorganisms present in the oral environment. This problem has been alleviated by the effective use of a solution of alkyl Di methyl benzyl ammonium chloride (Zephiran) in 1:750 concentration, in which the liners is soaked daily for 15 minutes after brushing with water.
Conclusion
The philosophy as presented here, as it must be for all dentistry, is that of conditioning and rejuvenation of traumatized tissue and maintenance and conservation of the healthy tissue. The applications of Elastomers in the prevention and treatment of chronic tissue irritation from dentures is an excellent alternative to the use of hard polymer resins and it is useful for preserving the health of the remaining denture supporting tissues.Wider applications will be found in the future, once the present short comings of the available materials are over come, whether by improving these materials or by developing new ones.So research must be continued in both existing and new materials in the hope- that the dental profession will see the development of clinically ideal soft denture lining material.
References
1. PHILLIPS, 11 th edition-Science of dental materials
2. Zarb And Bolender 12th edi,Prosthodontic treatment for edentulous patients
3. Sheldon Winkler 2nd edi,Essentials of complete denture Prosthodontics
4. Tissue conditioners; functional impressions; resilient liners. Coombe - Notes on dental materials.
5. Influence of lining design of three processed soft denture liners on cushioning effect J Oral Rehabil 1999: 26;962-968.
6. Soft lining materials in prosthetic dentistry;a review,Int J Prosthodont 1990: 3;477-483.
7. Complete dentures--the soft option. An update for general dental practice.Br Dent J 1997; 26;182:313-7.
8. Effects of viscoelastic properties of resilient denture liners on pressures under dentures,J Oral Rehabil 2001: 28;1003-1008.
9. Resilient materials for denture prosthesis- J Prosth Dent-1966; 16:438-42.
10. The compatibility of soft lining materials and denture cleansers—Br Dent J 1986; 161:13-17.
11. Soft lining materials: their absorption of, and solubility in, artificial saliva. Br Dent J 1988; 165:91-4.
12. The compatibility of temporary soft materials with immersion denture cleansers. Int J Prosthodont 1989; 2 : 254-8.
13. Creep and stress relaxation of soft denture liners. J Prosth Dent 1982; 48:135-40.
14. Water absorption and water solubility of soft lining materials for acrylic resins, J Den Res-1983; 62:764-768.
15. The plasticizing effect of temporary soft lining materials on polymerized acrylic resins. J Prosth Dent1988; 60:463-6.
16. Pros and cons of hard and resilient denture base materials.J Am Dent Assoc1977; 94:511-8.
17. Physical properties of tissue conditioning materials as used in functional impression. J Prosth Dent 1972; 27:111-9.
18. Tissue conditioning and tissue conditioners. Dent Clin North Am1975; 19:255-68.
19. Use of tissue conditioners and resilient liners. Dent Clin North Am1977; 21:249-59.
20. Resilient soft liners and tissue conditioners. Br Dent J 1988; 11:357-60.
21. Soft lining material in prosthetic dentistry- a review of literature. Int J Prosthodont1990; 5:477-88.
22. A contemporary update on 'soft' linings.-Dent Update2011;38(2):102-4.
23. Soft liners-Dent Clin North Am2004; (48):709-20
|