Introduction
Badly mutilated teeth or the grossly decayed teeth often pose problems to the restorative dentists during their treatment due to unavailability of sufficient clinical crowns. Hence a crown lengthening surgery prior to restorative treatment is mandatory during management of such teeth.
Crown lengthening is aimed at removal of periodontal tissue to increase the clinical crown height. To achieve this goal, one needs to have an understanding of biological width, indications, technique, as well as some possible limitations
Clinical crown lengthening refers to procedures designed to increase the extent of supragingival tooth structure for restorative or aesthetic purposes[1]. Clinicians often encounter the need for crown lengthening in the practice of dentistry and have to make treatment decisions taking into consideration how to best address the biological, functional, and aesthetic requirements of each particular case
The concept of tooth lengthening was first introduced by D.W. Cohen (1962)[2] and is presently a procedure that often employs some combination of tissue reduction or removal, osseous surgery, and / or orthodontics for tooth exposure. The amount of tooth structure exposed above the osseous crest (about 4mm) must be enough to provide for a stable dentogingival complex and biologic width to permit proper tooth preparation and account for an adequate marginal placement, thus ensuring a good marginal seal with retention for both provisional and final restorations [3].
This article discusses crown lengthening as one way in which the dentist can address both functional and aesthetic demands
Indications[1]
The indications for crown lengthening are:
• Restorative needs
• To increase clinical crown height lost due to caries, fracture or wear
• To access Subgingival caries
• To produce a ‘ferrule’ for post crown provision
• To access a perforation in the coronal third of the root
• To relocate margin of restorations that are impinging on biological width.
• Aesthetics
• Short teeth
• Uneven gingival contour
• Gummy smile.
Contra-indications & Limiting Factors[4]
• Inadequate crown to root ratio
• Nonrestorability of caries or root fracture
• Aesthetic compromise
• High furcation
• Inadequate predictability
• Tooth arch relationship inadequacy
• Compromising of adjacent periodontium or aesthetics
• Insufficient restorative space
• Nonmaintainability
Classification Of Aesthetic Crown Lengthening
Ernesto has proposed the following classification[5]:
Concept Of Biologic Width[6]
The concept of the biologic width first originated by research conducted by Garguilo, Wentz, and Orban where the distance between the apical end of the gingival sulcus and the crest of the alveolar bone was measured on several cadaver specimens[6],[7]. In areas that present with periodontal health, that distance, now regarded as the biologic width, was reported to be an average of 2.04 mm, where approximately 0.97 mm is occupied by the junctional epithelium and 1.07 mm is occupied by connective tissue attachment to the root surface. It has been shown the biologic width is approximately 2mm in 85 percent of population. In approximately 13 percent of the population, the distance exceeds 2mm while the same distance is less than 2mm in 2 percent of the individual’s examined[8]. The physiologic location of the biologic width can vary with age, tooth migration due to loss of arch or occlusal integrity, or orthodontic treatment.
Violation of the biologic width is a common occurrence in the practice of restorative dentistry. A familiar clinical situation in which the biologic width can be violated is by the placement of a deep subgingival restoration. The need to establish a subgingival restorative margin can be dictated by caries, tooth fracture, external root resorption, or the need to increase axial height of a tooth preparation for retention purposes.
If the apical margin of the restorative preparation is placed within the biologic width (i.e., too close to the bone), a zone of chronic inflammation is likely to develop[9]. One of the theories proposed is that there is insufficient space for a “normal” length junctional epithelium to develop; the functional epithelium is short, weak, and does not exert an effective sealing effect of the dentogingival unit[10]. Moreover, the area is easily damaged by mechanical oral hygiene practices, and chronic inflammation persists or is easily induced. Others believe a deeply placed subgingival restorative margin, close to the alveolar bone crest, impairs proper plaque control promoting inflammatory changes not conducive to a healthy periodontal environment[11].
Concept Of Supraosseous Gingiva
Some authors suggested that considering the total dentogingival complex rather than its individual components could eliminate the inherent errors in locating the base of the sulcus, suggesting the concept of supracrestal gingival tissue (SGT) that could dictate the amount of osseous resection required during crown lengthening.[12] The amount of bone resection required to accommodate the reforming supraosseous gingiva (SOG) and to expose sufficient healthy tooth structure for preparation has been considered to range from 3 to >5 mm.[3],[13],[14],[15]
According to literature, SGT is predetermined and that placing the FGM coronal to the osseous crest at the completion of crown-lengthening surgery could provide better guideline to the restorative dentist because the gingival tissue may take a more time to reach final height and contour. It has been established that suturing the flap >=3 mm from the osseous crest after crown-lengthening surgery resulted in insignificant tissue rebound. After surgery, there is a tendency for the formation of a new supracrestal gingival complex with its mean dimensions at 6 months found to be 0.45 mm less than those present before surgery. Therefore, preoperative SGT measurements formed after surgery may slightly overestimate the amount of exposed tooth structure desired. Hence, the osseous reduction to be performed may require additional considerations, such as tissue biotype, tooth type, and postoperative position of gingival margin in relation to osseous crest. The presence of thick biotype will require greater bone reduction as greater tissue rebound expected.[12] Regarding initiation of final prosthetic treatment, the final position of the free gingival margin can occur at three months after surgery but may occur as long as six months after surgery and for the areas in the esthetic zone, a waiting period of six months is advised.[16]
Treatment Options For Cls[17], [18]
Surgical
A. Gingivectomy
• Conventional ( Surgical)
• Laser
• Electrocautery
B. Internal Bevel Gingivectomy
C. Apical positioning of flap with or without ostectomy
Non Surgical - Orthodontic Treatment
Combined
Cls Using External Bevel Gingivectomy[17]
In the young adult with an intact periodontium the gingival margin normally resides about 1 mm coronal to the cemento-enamel junction. However, some patients may have a height of free gingiva that is greater than 1 mm, resulting in an unproportional appearance of the clinical crown. If such a patient complains about their “small front teeth” and the periodontium is of a thin biotype, full exposure of the anatomical crown can be accomplished by a gingivectomy/gingivoplasty procedure.
An assessment should also be made regarding the amount and pattern of pigmentation existing within the gingival tissues, and the patient's desire to maintain or lessen the pigmentation contained within the tissues. The externally beveled path of incision that is usually employed in a gingivectomy procedure will remove the pigmentation and produce pink gingival tissue upon initial healing. The surgically induced color change in the tissues comes about rapidly, and markedly affects esthetic values. For this reason, an externally beveled gingivectomy procedure should not be terminated at the midline in patients that have pigmented gingival tissues. It should be extended across the midline to the premolar area to avoid a color mismatch in the esthetic zone of the anterior teeth. The color change may be permanent or the pigmentation may slowly return over a period of a year or more. Patients should be informed of the changes in tissue color that will occur and should be allowed to make a choice as to the color of the tissue they will have post surgically. If they wish to maintain their pigmentation, an internally beveled path of incision (internal gingivectomy) should be employed.
Cls Using Internal Bevel Gingivectomy (Undisplaced Flap) [19]
The undisplaced flap and the gingivectomy are the two techniques that surgically remove the pocket wall. To perform this technique without creating a mucogingival problem, the clinician should determine that enough attached gingival will remain after removal of the pocket wall. The following steps outline the undisplaced flap technique.
Step 1- The initial or inverse bevel incision is made. The incision is usually carried to a point apical to the alveolar crest depending upon the thickness of the tissue or the pocket depth.
Step 2- The second or the crevicular incision is made from the bottom of the pocket to the bone to detach the connective tissue from the bone.
Step 3- The flap is then raised and third incision is given to remove the tissue tags
Step 4- After complete scaling and root planning flap is then sutured back in position
Cls Using Apically Positioned Flap1[19], [20] (Lindhe & Carranza)
One of the first authors to describe a technique for the preservation of the gingiva following surgery was Nabers (1954)[21]. The surgical technique developed by Nabers was originally denoted "repositioning of attached gingiva" and was later modified by Ariaudo & Tyrrell (1957)[22]. In 1962 Friedman[23] proposed the term apically repositioned flap to more appropriately describe the surgical technique introduced by Nabers. Friedman emphasized the fact that, at the end of the surgical procedure, the entire complex of the soft tissues (gingiva and alveolar mucosa) rather than the gingival alone was displaced in an apical direction. Thus, rather than excising the amount of gingiva which would be in excess after osseous surgery (if performed), the whole mucogingival complex was maintained and apically repositioned. This surgical technique was used on buccal surfaces in both maxillas and mandibles and on lingual surfaces in the mandible, while an excisional technique had to be used on the palatal aspect of maxillary teeth.
The apically positioned flap technique with bone recontouring (resection) may be used to expose sound tooth structure. As a general rule, at least 4 mm of sound tooth structure must be exposed at time of surgery. During healing the supracrestal soft tissues will proliferate coronaly to cover 2-3 mm of the root[24],[25] thereby leaving only 1-2 mm of supragingivally located sound tooth structure.
Indication : Crown lengthening of multiple teeth in a quadrant or sextant of the dentition.[17]
Contraindication : Surgical crown lengthening of single teeth in the esthetic zone.
Technique : According to Friedman (1962)[23] the technique should be performed in the following way:
An internal bevel incision is made. To preserve as much of the keratinized and attached gingival as possible, it should be no more than about 1mm from the crest of the gingival and directed to the crest of the bone. The incision is made after the existing scalloping, and there is no need to mark the existing scalloping and the bottom of the pocket in the external gingival surface because the incision is unrelated to pocket depth. It is also not necessary to accentuate the scallop interdentally because the flap is displaced apically and not placed interdentally. Then Crevicular incisions are made, followed by initial elevation of the flap, then interdental incisions are performed, and the wedge of tissue that contains the pocket wall is removed. Vertical incisions are then made extending beyond the mucogingival junction. It is important that vertical incisions, and thereafter the flap elevation, reach past the mucogingival junction to provide adequate mobility to the flap for its apical displacement. If the objective is a full thickness flap, it is elevated by blunt dissection with a periosteal elevator. If a split thickness flap is required, it is elevated using sharp dissection with a Bard- Parker knife to split it, leaving a layer of connective tissue, including the periosteum on the bone.
After removal of all granulation tissue, scaling and root planning, and performing osseous surgery if needed, the flap is displaced apically. If a full thickness flap was performed, a sling suture around the tooth prevents the flap from sliding to a position more apical that that desired, and the periodontal dressing can avoid its movement in a coronal direction. A partial thickness flap is sutured to the periosteum using a direct loop suture or a combination of loop and anchor suture. A dry foil is placed over the flap before covering it with the dressing to prevent the introduction of pack under the flap.
Sequence Of Treatment (Allen, 1993)[26]
Clinical and Radiographic Evaluation
1- Caries Control
2- Removal of Defective Restorations
3- Placement of Provisional Restorations
a. Control of Inflammation
b. Better Assessment of Crown Lengthening Required
c. Improved surgical access, especially interproximally
d. Enhanced predictability of margin placement post surgically
4- Endodontic therapy
a. Precedes surgery
b. If not possible, then completion is 4 to 6 weeks post surgically
5- Control of gingival inflammation
a. Plaque control
b. Scaling and root planing
6- Re-evaluation for
a. Orthodontic treatment
b. Surgical therapy
7- Surgery
Presurgical Analysis
Smukler and Chibi (1997)[27] recommended the following presurgical clinical analysis prior to crown lengthening procedures:
1- Determine the finish line prior to surgery
2- If non determinable, it should be anticipated
3- Transcrevicular circumferential probing prior to surgery is performed for establishing the biologic width (Bone Sounding)
a. Surgical site
b. Contra lateral site
4- The biologic width requirements will determine the amount of alveolar bone removal
5- The combination of biologic width and prosthetic requirements determines the total amount of tooth structure necessary for exposure
6- Tooth structure topography, anatomy, and curvature are analyzed for determining
a. Osseous scallop
b. Gingival form
Bone Sounding
The level of the alveolar crest must be determined prior to any considerations regarding aesthetic crown lengthening so as to determine the feasibility, surgical aspects, and treatment sequence
It is done following the administration of a local anesthesia, a measuring instrument is utilized to puncture and penetrate the mucosa until contact is made with the underlying bone. During this periodontal evaluation, bone sounding assists in determining the level of the alveolar crest and thus the need for osseous contouring[3], [28]
Specifically applied to aesthetic crown lengthening, bone sounding is performed in an attempt to determine the location of the alveolar crest, primarily on the labial aspect but additionally including the proximal areas. To this effect, a periodontal probe is inserted into the sulcus and forced to penetrate transgingivaly until contact is made with the alveolar crest, perforating the functional epithelium and gingival connective tissue in the process.
General Tissue Asseament Before Undetaking Cls
Soft Tissue Assesment
Situation 1 - If width of attached gingiva adequate (>3mm) - external bevel incision (gingivectomy)
Situation 2 - If width of attached gingiva inadequate (<3mm)- apically positioning flap
Hard Tissue Assesment
Situation 1- If bone crest is low i.e. more apically – no ostectomy
Situation 2- If bone crest is high i.e. more coronal- ostectomy performed
Ø Bone Crest Levels
A) Normal Crest
B) High Crest
C) Low Crest
• Low crest unstable- In this situation the gingival sulcus exaggerated, bone level is apical , less of attachment and thus less of biologic width
• Low crest stable- In this situation the gingival sulcus is normal with apical bone levels, more of attachment and therefore more of biologic width.
Case Report Series
This article would briefly describe various methods of performing CLS in different clinical situations through a series of 4 Case Reports
Various Methods described here are:
• INTERNAL BEVEL GINGIVECTOMY (Conventional Method)
• EXTERNAL BEVEL GINGIVECTOMY (Using Lasers)
• APICALLY POSITIONING OF FLAP WITH OSSEOUS RECONTOURING
• APICALLY POSITIONING OF FLAP WITHOUT OSSEOUS RECONTOURING
Crown Lengthening Using Internal Bevel Gingivectomy
A 23 year old male patient reported to the Department of Conservative Dentistry & Endodontics, SRDC, Faridabad, Haryana, with the chief complaint of broken tooth in upper front teeth region. Clinical examination revealed horizontal fractured tooth extending subgingivally in the palatal area of 12. Since the patient was young and wanted to save the tooth, the patient was checked and referred to Department of Periodontics for needful and the following treatment plan was formulated.
- Root Canal Treatment wrt 12
- Crown Lengthening Surgery wrt 12
- Prefabricated post & core build up
- Jacket Crown
Prior to crown lengthening procedure, a careful evaluation of location of bone as well as probing depth was done wrt 12. Bone sounding after administration of Local Anaesthesia was performed to rule out the necessity of osseous surgery. The pockets on each surface of 12 were explored with a periodontal probe. Evaluation of attached gingiva was also done using a periodontal probe. Upon examination following parameters were recorded:
1- Adequate amount of attached gingiva i.e. 3-4 mm on the buccal aspect
2- 3-4 mm of sulcular depth at all the six sites irt tooth 12
3- Low crest bone levels
With these factors in mind, in this case, internal bevel gingivectomy was performed using scalpel (conventional surgical method).
Surgery
Before undergoing surgery, presurgical analysis was done as already described above. (Smukler and Chibi (1997))
Step1- The surgical site was infiltrated with local anesthetic supplemented with epinephrine 1:80,000 to ensure sufficient anesthesia & haemostasis.
An adequate band of keratinized gingiva was clinically present along with low crest bone levels.
Step 2- With these factors in mind, an internal bevel incision was given using a 15 number blade followed by sulcular incision irt 12 from both the buccal and palatal aspect.
Step 3- Then a mucoperiosteal flap was fully reflected with a periosteal elevator, and the area was debrided thoroughly along with removal of tissue tags with the help of curettes and surgical knives.
At this point, using a periodontal probe sound tooth structure was measured from the crest of the alveolar bone which was around 4mm which was sufficient enough to give space for biologic width and sound tooth structure for the preparation of crown margins. Therefore there was no requirement of osseous surgery.
Step 4- Therefore the flap was thinned and sutured back in place using 3-0 black braided silk sutures followed by placement of periodontal dressing.
The patient was instructed to refrain from brushing, and a 0.12% chlorhexidine mouthwash was prescribed for use twice a day until mechanical tooth cleaning was resumed. Since a 5 day course of antibiotic was already given during the emergency phase, the antibiotics were not prescribed after surgery. A nonsteroidal anti-inflammatory drug was administered immediately after surgery and then again every 12 hours for 48 hours.
Healing
Sutures were removed after 7 days, and the healing was uneventful. Follow-up appointments occurred weekly until adequate patient hygiene was demonstrated. 3 weeks after the surgical procedure, the post space was prepared and prefabricated post was cemented and core build up was done. Crown preparation was done followed by Impression making and finally after all the laboratory procedures, Jacket crown was placed.
 | Figure 1 Pre-operative Of Internal Bevel Gingivectomy
 |
 | Figure 2 Post-operative Of Internal Bevel Gingivectomy
|
 | Figure 3 Pre-operative Of External Bevel Gingivectomy With Lasers
|
Gingivectomy Using Lasers[29]
Lasers have increasingly been used in modern dentistry for more than 30 years. A wide range of lasers such as CO2, Nd:Yag, and Er:Yag are used in the field of Periodontology for soft and hard tissue ablation, detoxification of root surfaces, pocket debridement, bacterial elimination and various surgical approaches[29]
Laser soft-tissue surgery has been shown to be well accepted. The greatest advantage of the laser is the lack of local anesthesia injection and the associated pre- and postoperative discomfort[30]. It may also enhance epithelisation and improve wound healing after gingivectomy and gingivoplasty operations[31]. In one of our procedures we used lasers for CLS.
A 25 year old male patient reported to the Dept of Conservative Dentistry & Endodontics, SRDC, Faridabad, Haryana, with the chief complaint of broken tooth in upper front teeth region. Upon clinical examination it was observed that there was a Horizontal fractured tooth extending subgingivaly in the palatal area of 12. Patient was then referred to department of Periodontics for needful
Upon examination following parameters were recorded:
1- 3-4 mm of sulcular depth at all the six sites with relation to tooth 12
2- Low crest bone levels
In this case, external bevel gingivectomy was decided to be performed using lasers
Surgery
Before undergoing surgery, presurgical analysis was done as already described above. (Smukler and Chibi (1997))
The surgical site was infiltrated with local anesthetic supplemented with epinephrine 1:80,000 to ensure sufficient anesthesia & haemostasis. 3-4mm of sulcular depth along with low crest bone levels were present. With these factors in mind, an external bevel gingivectomy was performed using lasers. After the patient preparation, the area was dried and then with the help of a diode laser gingivectomy procedure was performed. The charred tissue was continuously being cleared off with the help of moist gauze. Then a periodontal dressing was applied. The procedure was limited only to tooth number 12. Post surgically, the patient was given the same instructions as mentioned in previous case
Healing
Periodontal dressing was removed after 7 days, and the healing was uneventful. Follow-up appointments occurred weekly until adequate patient hygiene was demonstrated. 3 weeks after the surgical procedure, the post space was prepared and prefabricated post was cemented and core build up was done. Crown preparation was done followed by Impression making and finally after all the laboratory procedures, Jacket crown was placed.
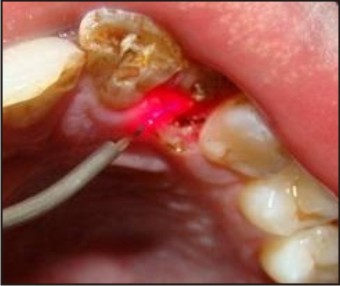 | Figure 4 Surgery Being Performed With Lasers.
|
 | Figure 5 Post-operative External Bevel Gingivectomy With Lasers
|
 | Figure 6 Pre-operative Of Apically Positioning Of Flap With Bone Contouring
|
Cls With Apical Positioning Of Flap With Osseous Recontouring
A female patient aged 30 yrs reported to the Dept of Prosthodontics, SRDC with the chief complaint of replacement of missing teeth and restoration for remaining teeth. On examination the upper and lower anterior teeth revealed short clinical crown length and was referred to Dept of Periodontics for crown lengthening.
Upon examination in the maxilla with the help of probing and bone sounding the following parameters were recorded:
Adequate width of attached gingival
High crest bone level
2-3 mm of sulcular depth
Short Clinical Crown Length
Therefore an apical positioning of flap was decided to be performed along with osseous recontouring in teeth no 11, 12 & 21 followed by crown fabrication by Department of Prosthodontics.
Surgery
After the presurgical analysis as described by Smukler and Chibi (1997) the steps 1 & 2 were performed as described in 1st case wrt to tooth number 11, 12 & 21. It was then followed by initial elevation of flap, then interdental incisions were performed, and the wedge of tissue that contains the pocket wall was removed. Vertical incisions were then made extending beyond the mucogingival junction. Then a full thickness flap was elevated by blunt dissection with a periosteal elevator. After removal of granulation tissue, scaling and root planning and osseous surgery using handpiece, burs and chisels, the flap was displaced apically and periosteal suturing was done using 3-0 black braided silk. A dry foil was then placed over the flap before covering it with the dressing to prevent the introduction of pack under the flap.
Patient was prescribed medications and instructed to maintain oral hygiene as instructed in 1st case.
Healing
Sutures were removed after 7 days, and the healing was uneventful. Follow-up appointments occurred weekly until adequate patient hygiene was demonstrated. 3 weeks after the surgical procedure, prosthetic part was undertaken and jacket crowns were placed.
 | Figure 7 Flap Reflection
|
 | Figure 8 Bone Contouring
|
 | Figure 9 After Bone Contouring
|
 | Figure 10 Post-operative Of Apically Positioning Of Flap With Bone Contouring
|
 | Figure 11 Pre-operative Of Apically Positioning Of Flap Without Bone Contouring
|
Cls With Apical Positioning Of Flap Without Osseous Recontouring[4], [23]
A female patient aged 30 yrs reported to the Dept of Prosthodontics SRDC with the chief complaint of replacement of missing teeth and restoration for remaining teeth. On examination the upper and lower anterior teeth revealed short clinical crown length and was referred to Dept of Periodontics for crown lengthening.
Upon examination in the mandible with the help of probing and bone sounding the following parameters were recorded:
- Adequate width of attached gingival
- Low crest bone level
- Short Clinical Crown Length
Therefore an apical positioning of flap was decided to be performed without osseous recontouring in teeth no 31, 32, 41 & 42 followed by crown fabrication by Department of Prosthodontics.
Surgery
After the presurgical analysis as described by Smukler and Chibi (1997) the steps 1 & 2 as described in 1st case were performed wrt to tooth number 31, 32, 41, & 42. It was then followed by initial elevation of flap, then interdental incisions were performed, and the wedge of tissue that contains the pocket wall is removed. Vertical incisions were then made extending beyond the mucogingival junction. Then a full thickness flap was elevated by blunt dissection with a periosteal elevator followed by split thickness using a Bard-Parker knife to split it, leaving a layer of connective tissue, including the periosteum on the bone. After removal of granulation tissue, scaling and root planning, the flap was displaced apically and periosteal suturing was done using 3-0 black braided silk. A dry foil was then placed over the flap before covering it with the dressing to prevent the introduction of pack under the flap.
Patient was prescribed medications and instructed to maintain oral hygiene as instructed in 1st case.
Healing
Sutures were removed after 7 days, and the healing was uneventful. Follow-up appointments occurred weekly until adequate patient hygiene was demonstrated. 3 weeks after the surgical procedure, the prosthetic part was undertaken and jacket crowns were placed.
 | Figure 12 Incisions
|
 | Figure 13 Suturing
|
 | Figure 14 Post-operative Of Apically Positioning Of Flap Without Bone Contouring
|
Discussion
Crown Lengthening is a surgical procedure that requires exposure of adequate tooth structure for restorative procedures. The cases discussed here have been treated with various techniques and methods. In all cases discusses here were treated in such a way so as to avoid any violation to Biologic Width that can have deleterious effect on periodontium leading to gingival inflammation, loss of attachment and alveolar resorption.
The goal of surgical crown lengthening is to provide the restorative dentist with sufficient clinical crown to permit optimum restoration of a tooth. The indications of surgical crown lengthening are subgingival caries, subgingival fracture, teeth shortened by extensive caries or fracture, naturally short clinical crown due to non exposure of anatomic crown.
The techniques of surgical crown lengthening are:
a- Internal Bevel Gingivectomy
b- External Bevel gingivectomy
c- Apically positioned flap with Bone Reduction
d- Apically positioned flap without bone reduction
In the cases described here, all the four procedures have been performed as per the requirement of the case. To perform these techniques various criteria are first required to set and then one should choose for an optimal technique which would best suit the situation . All the hard tissue and soft tissue parameters should be recorded first to evaluate the requirement of the case. For example in the first case described here, had sufficient amount of attached gingival as well as sulcular depth, thus an internal bevel gingivectomy procedure was performed. In one of the cases, there was sufficient amount of attached gingiva, and the crest of bone was low, therefore an apical positioned flap was done without osseous surgery and in one of the case there high crest bone level therefore an apical position flap with bone reduction was done. Thus these cases clearly describe various aspects of crown lengthening.
There are also various means of performing CLS, for example, Scalpels, Cautery and lasers. Here we have used scalpels and lasers. It has been seen that healing with lasers is faster than scalpels. Also post operative discomfort is lesser with lasers as compared with scalpels[31].
In the above discussed cases, various restorative and prosthetic procedures were performed once the crown lengthening was completed and have been shown to be clinically successful, thereby completing the rehabilitation of the patient.
Conclusion
Crown lengthening is as a viable procedure that enables to restore teeth having a short clinical crown, extensive subgingival caries, subgingival tooth fractures at dentogingival junction, when performed in ideal clinical conditions, crown lengthening gives satisfactory results both from a functional as well as aesthetic point of view.
References
1. Camargo PM, Melnick PR, Camargo LM . Clinical Crown Lengthening in Esthetic Zone. C D A Journal . 2007; 35(7) :487- 498
2. Cohen DW. Lecture, Walter Reed Medical Center 1962 June 3
3. Ingber FJS, Rose LF, Coslet JG. The biologic width - A concept in periodontics and restorative dentistry. Alphan Omegan 1977; 10:62-5
4. Cohen ES. Crown lengthening. Atlas of Cosmetic & reconstructive periodontal surgery. Third edition.
5. Ernesto A. Lee, Cir Dent. Aesthetic Crown Lengthening: Classification, Biologic Rationale, And Treatment Planning Consideration .Pract Proced Aesthet Dent. 2004; 16(10): 769- 778
6. Gargiulo AW, Wentz FM, Orban B. Dimensions and relations of the dentogingival junction in humans. J Periodontol. 1961;32:261-7
7. Cohen DW. Current approaches in periodontology. J Periodontol 1964;35:5-18
8. Kois J. The restorative-periodontal interface: biological parameters. Periodontology 2000, 1996; 11:29-38
9. Gunay H, Seeger A, et al. Placement of the preparation line and periodontal health- a prospective two-year clinical study. Int J Periodontics Restorative Dent. 2000; 20:171-81
10. Schroeder HE, Listgarten MA. Fine structure of the developing epithelial attachment of human teeth. Monogr Dev Biol. 1971;2:1-134
11. Holmes JR, Sulik WD, et al. Marginal fit of castable ceramic crown. J Prosthet Dent. 1992; 67:594-9
12. Arora R, Narula SC, Sharma RK, Tewari S. Evaluation of Supracrestal Gingival Tissue After Surgical Crown Lengthening: A 6-Month Clinical Study. J Periodontol. 2013 Jul;84(7):934-40.
13. Perez JR, Smukler H, Nunn ME. Clinical evaluation of the supraosseous gingivae before and after crown lengthening. J Periodontol. 2007;78:1023-1030
14. Becker W, Ochsenbein C, Becker BE. Crown lengthening: The periodontal-restorative connection. Compendium 1998;19:239-254
15. Rosenberg ES, Cho S, Garber DA. Crown lengthening revisited. Compend Contin Educ Dent 1999;20: 527-542
16. Timothy J. Hempton and John T. Dominici . Contemporary crown-lengthening therapyA Review .JADA 2010;141(6):647-655
17. Wennstrom J L, PiniPrato GP. Mucogingival therapy-periodontal plastic surgery; Clinical Periodontlogy & Implant dentistry. 4th edition
18. HH Takei. Preparation of the periodontium for restorative dentistry. Clinical Periodontology. Tenth Edition.
19. Carranza FA, Takei HH. The flap Technique for Pocket Therapy. Clinical Periodontology. Tenth Edition.
20. Wennstrom JL, Heijl L, Linde J. Periodontal Surgery: Access Therapy. Clinical Periodontlogy & Implant dentistry. 4th edition.
21. Nabers, CL. Repositioning the attached gingival. J Periodontol 1954; 25, 38-39
22. Ariadu, A.A , Tyrell, HA . Repositioning & increasing the zone of attached gingival. J Periodontol 1957; 28, 106-110
23. Friedman N. Mucogingival surgery. The apically repositioned flap. J Periodontol 1962.33: 328-340
24. Herrero F, Scott JB, Maropis PS, Yukna RA. Clinical comparison of desired versusactual amount of surgical crown lengthening. J Periodontol 1995; 66:568-571
25. Pontoriero R, Carnevale G. Surgical crown lengthening. A 12 month clinical wound healing study. J Periodontol 2001; 72: 841- 848
26. Allen EP.Surgical crown lengthening for function and esthetic. DCNA 1993; 37:163-79
27. Smukler H, Chaibi M. Periodontal and dental considerations in clinical crown extension. A rational basis for treatment. Int J Periodontics Restorative Dent 1997; 17:464-77
28. Kois JC. Altering gingival levels: The restorative connection. Part I: Biologic variables. J Esthet Dent 1994;6(1):3-9.
29. Cobb, C. M. Lasers in periodontics: a review of the literature. JOP 2006 77, 545–564
30. Kelman MM, Poiman DJ, Jacobson BL. Laser gingivectomy for pediatrics. A case report. N Y State Dent J. 2009 Jun-Jul;75(4):26-9
31. Ozcelik O, Haytac MC, Kunin A, Seydaoglu G. Improved wound healing by low-level laser irradiation after gingivectomy operations: a controlled clinical pilot study. J Clin Periodontol 2008; 35: 250–254
|