Introduction
Hypohidrotic ectodermal dysplasia is a rare genetic disorder characterized by dysplasia of tissues of ectodermal origin with a frequency varying between 1:10,000 and 1:1,00,000 live births and is more frequent in males. Fereire –Maia[4] defined ectodermal dysplasia as any syndrome that demonstrated at least two of the following features: trichodysplasia (abnormal hair) hypodontia / anodontia (abnormal dentition) , palmoplantar hypohidrosis (abnormal or missing sweat glands) , onchodysplasia (abnormal nails). Hypohydrotic Ectodermal dysplasia, also termed as Christ-Siemens Tourine syndromeis more common and is characterized by a triad of signs comprising[1]. sparse hair (hypotrichosis), [2]. abnormal or missing teeth (hypodontia or anodontia), and [3]. inability to sweat because of the lack of sweat glands (anhidrosis or hypohidrosis). Typical general mental development, frontal bossing with characteristics reduction in amount of hair (hypotrichosis), absence of sweat glands (anhidrosis) resulting in temperature elevation, absence of sebaceous glands (asteatosis) resulting in dry skin, depressed nasal bridge, protuberant lips, prominent supra orbital ridges , sunken cheeks, wrinkled hyperpigmented skin around the eyes and large low set ears[5]. The oral manifestations include conical or peg shaped teeth, hypodontia (partial absence of teeth) or complete anodontia (complete absence of teeth) of both the deciduous and the permanent dentition with malformation of any teeth that may be present, generalized spacing, underdeveloped alveolar ridges and delayed eruption of permanent teeth.
Case Report
A 28 year old male reported to the Department of Prosthodontics, Bhojia Dental College, Baddi with a complaint of missing and unaesthetic teeth. The patient exhibited the classical features of ectodermal dysplasia : hypodontia, hypohidrosis,hypotrichosis, prominent forehead, saddle nose, diminished lower facial height, sparse scalp hair, missing eyelashes, sparse eyebrows and protuberant lips. (Fig 1)
 | Fig 1 : Pre-operative Photograph
 |
Intra oral examination revealed (Fig 2).
1. Missing permanent lateral incisors and premolars in all the quadrants.
2. The permanent central incisors and canines were hypoplastic and conical in shape.
3. Malformed molars
4. Presence of Supernumerary teeth palatal to maxillary molars.
5. Edentulous areas were deficient in height and width.
6. Oral mucosa had a dry appearance.
 | Fig 2 : Intra Oral View
|
Occlusal analysis revealed class I molar occlusal relation on both right and left quadrants.
Radiographic examination revealed absence of permanent lateral incisors and premolars along with underdeveloped maxillary and mandibular ridges. (Fig 3).
 | Fig 3 : Radiographic View
|
Since hypohidrosis (inability to sweat), hypotrichosis (abnormal hair), and hypodontia (partial absence of teeth) were very evident on physical examination, the patient was diagnosed with Hypohidrotic Ectodermal Dysplasia (HED) with hypodontia.
Prosthodontic management
The prosthodontic management in patients suffering from Hypohidrotic Ectodermal Dysplasia depends on the degree of anodontia/hypodontia. In case of complete anodontia, the treatment would comprise of complete dentures, either conventional or implant supported ones. In patients with partial anodontia, removable/fixed partial dentures and over dentures may be considered.
In the present case, individual Porcelain Fused to Metal crowns were planned for the maxillary and mandibular anterior teeth and removable partial denture for the edentulous posterior area. Supernumerary teeth were not extracted as they served as an aid in retention of maxillary denture.
Esthetic re-contouring ofmaxillary and mandibularanterior teeth was done using light cure composite material.(Fig 4) They were used as guide for the final prosthesis.
 | Fig 4 : Recontouring Of Teeth With Composite Resin
|
Tooth preparations for the final prosthesis were done only after getting the approval of the esthetics by the patient. Tooth preparations of anterior teeth with knife edge finish lines were selected, although not recommended, to preserve tooth structure and to permit a little overcontouring in already thin, conical crowns.Porcelain Fused to Metal crowns were fabricated and cemented with resin bonded cement after taking the impressions in rubber base material(Fig 5). After the cementation of Porcelain Fused to Metal crowns, impressions were again made in rubber base impression material.
 | Fig 5 : Porcelain Fused To Metal Crowns
|
Final casts were made and bite rims prepared. Jaw relations were recorded and arrangement of posterior teeth done. Interim removable partial dentures were fabricated and inserted in the patient’s mouth (Fig 6,7). Removable partial dentures not only improved the esthetics and chewing ability but also allowed the patient to get accustomed to the raised vertical dimension. The final prosthesis planned are the cast partial dentures which will be given to the patient after he gets accustomed to the raised vertical dimension.
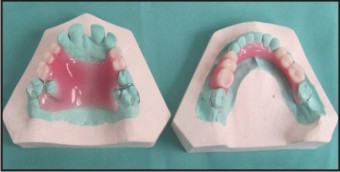 | Fig 6 : Removable Partial Dentures
|
 | Fig 7 : Post Operative View
|
Discussion
Prosthodontic treatment may commence at an early age as it enhances conditions for growth and development of orofacial structures. It helps normalize the function of masticatory and perioral muscles and consequently the growth pattern of basal bones and gives a psychological boost to the self-image of the person. Numerous clinical reports have demonstrated the importance of prosthetic dental treatment in Ectodermal Dysplasia patients for physiologic and psychosocial reasons.[6] A multidisciplinary team approach to treatment is recommended in these cases. Prosthodontic management of Ectodermal Dysplasia patient includes fabrication of complete or partial removable prosthesis, overdentures with or without tooth preparation,or overdentures with or without attachments and fixed partial denture prosthesis[7]. Osseo-integrated implants are an alternative treatment in older people with ectodermal dysplasia.[8],[9],[10] Considering the bone density,knife edge ridges and financial status of the patient, osseointegrated implants were precluded in the present case.[11] Anterior teeth were restored with individual porcelain fused to metal crowns because of generalized spacing present between them. Conventional interim removable partial dentures have proven to be advantageous in patients who have severely atrophic alveolar ridges. Therefore, removable partial dentures were the choice of treatment modality for the maxillary and mandibular posterior edentulous areas. Complete mouth rehabilitation resulted in improvement of the function, esthetics, and the psychosocial confidence of the patient.
Conclusion
The use of interim removable prosthesis is an interesting and practical alternative that provides a relatively quick, easy, acceptable and economical solution to the functional and esthetic oral rehabilitation in patients with pronounced edentulism. This solution improves the patient’s quality of life and optimizes social integration; furthermore, it permits stimulation of the alveolar ridges for later treatment with an implant supported prosthesis as a more stable and esthetic solution for patients with multiple dental agenesis.
References
1. Luiz, Gutenberg TM Coelho, Junior et al. Christ Siemens Touraine syndrome: a case report.Cases J. 2009; 2: 38.
2. Shaw RM. Prosthetic management of hypohidrotic Ectodermal dysplasia with anodontia. Case report. Aust Dent J 1990; 35; 113-116.
3. Hassed SJ, Kincannon JM, Arnold GL. Clouston syndrome: an ectodermal dysplasia without ssignificant dental findings. Am J Med Genet. 1996;61(3):274-6.
4. Freire-Maia N, Lisboa-Costa T, Pagnan NAB. Ectodermal dysplasias: how many? Amer J Med Genet. 2001;104:84.
5. Crawford PJ,Alred MJ,Clarke A. Clinical and radiographic dental findings in X- linked hypohidrotic ectodermal dysplasia. Journal of Medical Genetics, 1991; 28:181-185
6. Lowry RB, Robinson GC, Miller JR. Hereditary ectodermal dysplasia. Symptoms, inheritance patterns, differential diagnosis, management. Clin Paediatric 1966;5:395-402.
7. Guna S,Alluri R,Chandrasekhar R. Prosthetic rehabilitation of a patient with hypohidrotic ectodermal dysplasia:a clinical case. Braz J Oral Sci. 2010;9(1):63-66.s
8. Lakomski J, Kobielak, Kobielak A, TrZeciak WH. Correcting facial dysmorphism in a patient with anhidrotic ED- A clinical report. J Prosthet Dent. 1998;80:524-6.
9. Escobar V, Epker BN. Alveolar bone growth in response to endosteal implants in two patients with ED. Int J Oral Maxillofac Surg. 1998;27:445-7
10. Pae A, Kim K, Kim HS, Kwon KR. Overdenture restoration in growing patient with hypohidrotic ED- A clinilal report. Quintessence Int.2011;42:235-8
11. Lowry RB, Robinson GC, Miller JR. Hereditary ectodermal dysplasia. Symptoms, inheritance patterns, differential diagnosis, management. Clin Paediatric 1966;5:395-402.
|