Introduction
Restoration of fractured teeth needs ultimate care and preparation planning to assure that the remaining tooth structure is given maximum strength. The fracture resistance of such teeth is directly related to the remaining dentine thickness, especially in bucco-lingual direction.[1]
The cast metal post and core has been the time honoured method of restoring the endodontically treated teeth. But cast post and core has inordinately high failure rate in the form of root fracture, post dislodgement, cement failure or post fracture.[2],[3] Thecorrosion products, due to dissimilar metals in the post, core and crown could be the causative factor in the form of fracture of endodontically treated teeth. Besides this, cast post and core, has objectionable aesthetics; removes additional tooth structure; involves additional laboratory time and cost; is technique sensitive; may cause hypersensitivity (Ni-allergy); and has difficult retrieval.[4]
Most of the time endodontically treated teeth are weak for so many reasons like previous caries, trauma, old restorations, and even endodontic therapy in itself weakens the tooth.[7] The selection of the post system should be such that it offers maximum retention to core and yet removes as little dentine as possible.
The treatment goals for an endodontically treated tooth must be based upon factors specific for each patient that include occlusion, patient function, tooth position, periodontal status, prosthetic needs, economics, amount of remaining viable tooth structure, and root morphology.
To circumvent these problems, glass fiber-reinforced composite posts, and quartz fiber posts were introduced. These posts have the advantages of being highly esthetic, less incidence of post or root fracture, and have better retention, as post is actually bonded to tooth structure rather than cemented.
Also these posts are biocompatible, saves clinician’s time, and easy to place.[5], [6]
This article presents a case report in which excessively widened canal was narrowed using light transmitting plastic post and successful restoration of function and esthetics was achieved by using glass fiber post and composite core and final PFM crown in a patient of broken front tooth.
Clinical Case
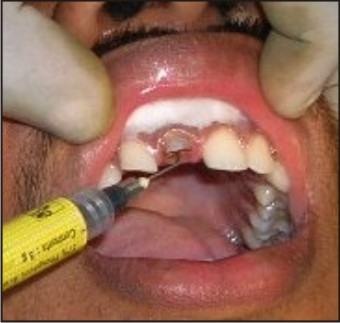
A patient aged 18 years, reported to the department of prosthodontics with the chief complaint of upper front tooth broken and discoloured. History of his present complaint revealed the trauma to left maxillary incisors due to fall from the bicycle 11/2 years back. Clinical evaluation revealed Ellis class III fracture in 11 and Class II fracture in 12 (Figure 1). Root canal therapy was done in 11 few months after the trauma and the tooth was asymptomatic. The canal was inordinately wide due to iatrogenic dentistry that he underwent somewhere else, however apical seal was satisfactory.
 | Figure 1
 |
The canal was very much widened near the access cavity (Figure 2). The diameter of the canal was calculated to be 4.3mm mesio-distally and 2.1mm bucco-palatally, which was much more than the recommended post diameter of 1.7mm in central incisor.
 | Figure 2
|
It was planned to narrow the canal with flowable composite using light transmitting plastic post to the desired diameter and then finally restoring the canal with glass fiber post using dual cure resin cement and PFM crown. Patient was informed of the necessary treatment and consent was taken.
Post space was prepared using Peeso reamers and Gates Glidden drills, leaving 5mm of apical gutta-percha. The caries near the access orifice was removed using slow speed micromotor, taking care not to further increase the canal diameter. The canal was irrigated with 2.5% NaOCl for 1 minute and finally rinsed with distilled water and dried.
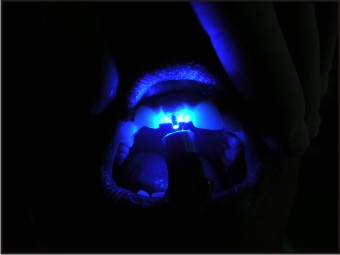
Light transmitting plastic post (Dentatus, USA) of diameter 1.7mm was chosen to narrow the widened canal. The post space walls were etched with 37% Phosphoric acid gel that was introduced into the canal with the needle (Figure 3) and after 30 seconds it was rinsed with distilled water and thoroughly dried with chip blower and paper points until no visible blue color and moisture could be observed. A bonding agent was applied gently into the canal using super fine micro brush, excess was removed using paper points, the adhesive was gently air dried for 5 seconds and light cured for 30 seconds. The canal was filled with flowable composite and light transmitting plastic post was introduced into the canal (Figure 4). It was light cured for 60 seconds through the cervical portion of the root and after that the plastic post was removed. The canal diameter was again measured and calculated to be 1.7mm.
 | Figure 3
|
 | Figure 4
|
The glass fiber post of diameter 1.7mm was selected and tried into the canal and marked 10mm according to the post space (Figure 5). The excess was sectioned with water cooled diamond rotary cutting instrument (R879.014; Diaswiss, Geneva, Switzerland) at high speedto avoid separation of glass fibers from its resin matrix. The IOPA X-ray was taken to confirm the snugly fit of the post. The canal was again washed with distilled water and dried with paper points. The acid etching was done again for 30 seconds and thoroughly washed and dried. The post was also etched for the purpose of cleaning, then rinsed and dried according to manufacturer’s instructions. The bonding agent was applied into the canal and onto the glass fiber post and cured for 20 seconds. The dual cure resin cement was mixed according to manufacturer’s instructions and applied into the canal using Lentulo spiral and also over the post surface. The glass fiber post was introduced into the canal to the full depth and kept under finger pressure for 1 minute. Then it was light cured for 60 seconds with the tip of the light curing unit in direct contact with the coronal end of the post. The core build-up was done with composite in increments which were light cured for 20 seconds each time and shaped with slow speed burs using a micromotor (Figure 6).
 | Figure 5
|
 | Figure 6
|
The crown preparation was done for PFM crown. An impression was made in polysiloxane using putty wash technique and sent to the laboratory for fabrication of PFM crown.
The temporary crown was cemented with non-eugenol cement. After two weeks, the completed PFM crown was luted with GIC cement. The broken Incisal edge of 12 was build up with composite of appropriate shade (Figure 7). The patient was happy and satisfied with the final work.
 | Figure 7
|
Discussion
The successful treatment of a badly broken down tooth with pulpal disease depends not only on good endodontic therapy but also on good prosthetic reconstruction of the tooth after endodontic therapy is completed. The most important consideration in the long term success of post retained restoration is the resistance form which largely depends upon the amount of remaining dentine in the canal, and also the tooth structure above the crown margin. Thus, the amount of theremaining tooth structure dictates the type of therestoration that should be given inpulpless teeth.[7]
In this case, the diameter of the root canal was not favourable to place any post for certain reasons:
1. The remaining dentine thickness was very less.
2. The post space preparation would itself lead to dentine removal and further weakening of the tooth.
3. No prefabricated post of that size was available in such a wide canal.
4. Custom cast post could further weaken the tooth and lead to its fracture.
So, it was decided to narrow the canal to appropriate diameter. Attempts have been made in the past to restore the widely canalled tooth by narrowing it with flowable composite using light emitting post.[8],[9] As the tooth had a very weak canal due to much loss of dentine all around, the custom cast post will further weaken the tooth because of greater rigidity and stress concentration in the canal.
The post material should have its modulus of elasticity comparable to that of dentine to prevent stress concentration and subsequent fracture of the tooth or the post.[10] The glass fiber post has MOE similar to that of dentine and resin cement and composite core will lead to formation of a“Monobloc.”[6]
This technique has advantage of reinforcing internally the weakened narrow root canal with composite that adapts well with its walls, thus offering maximum shear load support and retention.
Summary
For flared root canals, light transmitting plastic posts can be used to narrow their diameters within the acceptable range of restoration using flowable composites that reinforce internally the weakened root canal. Glass fiber posts of appropriate diameter then can be used as final post over which composite core build up can be done so that a Monobloc is constituted. Dual cured adhesive cements give assurance of their complete polymerization in the depths of the root canals. All these if inosculated wisely can save a badly mutilated tooth from extraction as evident in this case report.
References
1. Gutmann JL. The Dentin-Root Complex: Anatomic and biologic considerations in restoring endodontically treated teeth. J Prosthet Dent 1992; 67: 458-67.
2. Morgano SM and Milot P. Clinical success of cast posts and cores. J Prosthet Dent 1993; 69: 11-16.
3. Sorenson JA and Martinoff JT. Clinically significant factors in dowel design. J Prosthet Dent 1984; 52: 28-35.
4. Robbins JW. Guidelines for the restoration of endodontically treated teeth. J Am Dent Assoc 1990; 120: 558-66.
5. Ferrari M, Vichi A and Garcia Godoy F. Clinical evaluation of fiber-reinforced epoxy resin posts and cast post and cores. Am J Dent 2000; 13: 15B-18B.
6. Pest LB, Cavalli G, Bertani P, and Gagliani M. Adhesive post-endodontic restorations with fiber posts: push-out tests and SEM observations. Dent Mater 2002; 18: 596-602.
7. Assif D and Gorfil C. Biomechanical considerations in restoring endodontically treated teeth. J Prosthet Dent 1994; 71: 565-67.
8. LA Conclaves, LPV Vansan, SM Paulino, MS Neto. Fracture resistance of weakened roots restored with a transilluminating post and adhesive restorative materials. J Prosthet Dent 2006; 96:339-44.
9. Lui, J.L Composite Resin Reinforcement of Flared Canals Using Light-Transmitting Plastic Posts. Quintes Intern 1995; 25: 320-25.
10. Cormier CJ, Burns DR and Moon P. In-vitro comparison of the fracture resistance and failure mode of fiber, ceramic and conventional post systems at various stages of restoration. J Prosthodont 2001; 10: 26-36.
|