Introduction
Acquired defects of the maxilla may result from pathological changes, trauma, or after surgical resection of oral neoplasms. These defects pre-dispose the patient to difficulty in swallowing, mastication, fluid leakage into the nasal cavity and hypernasal speech[1].
Rehabilitation of these defects not only improves speech, swallowing and mastication, but also it has a great role in improving the quality of patients life[2]. Oral rehabilitation of patients with acquired defects of the maxilla present a challenging task for the maxillofacial prosthodontist. Compromised support, retention, stability and weight of the prosthesis are common prosthodontic treatment problems for these patients.
In partially edentulous patients support, stability and retention of a removable obturator prosthesis relies on the remaining hard and soft tissues[2],[3]. The larger the surgical resection, the greater the loss of the mucogingival support, which in turn results in increased unfavourable forces acting on the remaining abutment teeth[4]. Reducing the weight of the prosthesis is important for retention [3],[4],[5]. Many techniques for hollow obturators have been documented in the literature[6],[7],[8],[9]. This clinical report demonstrates a new technique for the fabrication of hollow maxillary resection prosthesis for decreasing the weight of the prosthesis for a patient with right side maxillectomy.
Case Report
A 31 year-old female patient presented with a chief complaint of difficulty in speech and deglutition of one and a half year’s duration. Patient had undergone surgery for adenoid cystic carcinoma of palatal salivary glands of the right maxilla. Intraoral examination revealed maxillectomy of the right side along with removal of zygomatic bone of the same side. Maxillary left central incisor (21) was also missing(Figure 1). The presented defect corresponded to the Aramany’s Class I situation[4],[5]. Buccal mucosa of right side was pulled medially and was sutured to the mid palatine raphe by the surgeon in an attempt to close the defect. But there was oro-nasal communication due to necrosis of some part of the mucosa. Patient was advised to undergo a surgical procedure, so that this buccal flap can be released and defect can be opened up completely, for better esthetics and stability of the prosthesis, but patient was not willing for any more surgical procedures.
 | Figure 1 : Intra Oral View Of The Defect.
 |
The mandibular arch was completely dentulous. Mandibular movements were within the normal range, with no evidence of supraeruption of mandibular teeth. Tongue function was normal and speech was altered. Considering stability, retention, load distribution and supra structure longevity, the decision was made to rehabilitate the patient with a cast partial maxillary resection prosthesis [10].
Procedure
• Primary impressions were made using irreversible hydrocolloid impression material (Tropicalgin;Zhermack, Italy) after blocking the defect with the gauze.
• After surveying the cast, designing of the cast partial denture was done[10]. Combination clasps were planned on 24,25,26 and 27, I bar on 22 and proximal plate on mesial aspect of 22.
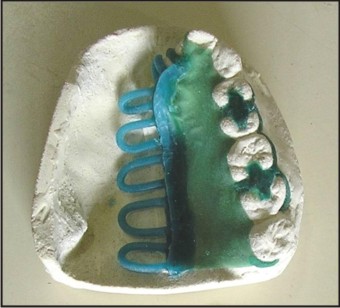
• Rest seat preparation was done on 24,25,26 and 27. Guide planes preparation done on 22. Border molding of the resected region was done using greenstick compound , and a complete arch impression was then made using addition polyvinyl siloxane impression material. (Aquasil soft putty,Dentsply Caulk, USA, Aquasil Ultra XLV / Regular set ,Dentsply Caulk, USA) (Figure 2). Master cast was blocked out, duplicated and wax pattern was made[10] (Figure3). Cast metal framework was fabricated and checked intraorally for retention.
• Permanent record base of (1.5 mm thickness) was made using heat cure acrylic resin(DPI Heat CureTM, Dental products of India Ltd.) (Figure 4), bite registration was done, teeth arrangement was followed by trial and acrylization was done (Figure 5).
• Using a acrylic bur , a hole was made on the denture base and obturator bulb was hollowed out from inside (Figure 6).
• Base paste of addition polyvinyl siloxane impression material ,putty consistency, (Aquasil hard putty, Dentsply Caulk, USA,) was used to fill up the polished surface of the record base to bring it to the correct palatal contours.
• On this base paste, a lid of modelling wax(DPI Modelling wax, Dental products of India Ltd.) was formed to simulate the corrected palatal contours (Figure 7). Wax lid was carefully removed for the prosthesis, invested and acrylized in heat polymerized acrylic resin (Figure 8). This acrylic lid was then attached to the prosthesis using auto polymerising acrylic resin ( DPI-RR Cold CureTM, Dental products of India Ltd.) (Figure 9). Prosthesis was kept in water for 48 hrs to remove any residual monomer. Thus the weight of the prosthesis was reduced.
• Post insertion follow-up and patient care were carried out for a period of one year, which revealed that the patient was satisfied and comfortable with the functioning of the prosthesis.
 | Figure 2 : Final Impression After Border Molding The Defect Area.
|
 | Figure 3 : Wax Pattern Made On Duplicated Cast.
|
 | Figure 4 : Permanent Record Base Fabricated.
|
 | Figure 5 : Acrylized Denture With Under Contoured Palatal Area.
|
 | Figure 6 : Obturator Bulb Hollowed Out.
|
 | Figure 7 : Lid Of Modelling Wax Applied On The Base Paste Of Addition Polyvinyl Siloxane Impression Material, To Achieve Correct Palatal Contours.
|
 | Figure 8 : Acrylized Wax Lid.
|
 | Figure 9 : Final Hollow Maxillary Resection Prosthesis.
|
Discussion
Obturator prostheses are commonly used in the rehabilitation of total or sub-total maxillectomy patients, as it helps in separating the oral and the nasal cavities and restores normal deglutition and speech and further improves the mid-facial aesthetics by supporting the soft tissues[2],[3].
Reducing the weight of the prosthesis is an important aspect of the treatment. Many techniques of hollowing the obturator are mentioned in the literature[6],[7],[8],[9]. In this case report, not only the bulb of the obturator is hollowed out , but also the area of the prosthesis replacing the palate. This article presents a simple and predictable approach for fabricating a hollow maxillary resection prosthesis, as compared to other techniques[4],[5],[6],[7],[8],[9] that use salt, sugar, asbestos or other silicone rubber foams as obturating material, that can be technique sensitive, unstable and dangerous.
Summary
Prosthetic rehabilitation of the dentate maxillectomy patient is a lengthy and time involved process. Hollow maxillary resection prosthesis aids in better retention by decreasing the weight and thus improves patient compliance. This case report describes an innovative technique to fabricate a hollow maxillary resection prosthesis. This technique is simple and predictable results can be obtained.
References
1. Beumer J, Curtis T, Marunick M. Maxillofacial rehabilitation: prosthodontic and surgical considerations. St Louis: Ishiyaku EuroAmerica, Inc.;1996.p.399-402.
2. Lang BR,Bruce RA. Presurgical maxillectomy prosthesis. J Prosthet Dent 1967;17(6):613-9.
3. Parr GR. Prosthodontic principles in the framework design of maxillary obturator prosthesis. J Prosthet Dent 1989;62(2):205-12.
4. Aramany MA. Basic principles of obturator design for partially edentulous patients Part I: Classification. J Prosthet Dent 1978;40: 554-57.
5. Aramany MA. Basic principles of obturator design for partially edentulous patients Part II: Design principles. J Prosthet Dent 1978;40:656-62.
6. Eric SA, Jason JP, John DP, Robert FW. Technique for quick conversion of an obturator into a hollow bulb. J Prosthet Dent2001;85(4):401-8.
7. Mc Andrew KS, Rothenberger SL, Minsley GE. An innovative investment method for the fabrication of a closed hollow obturator prosthesis. J Prosthet Dent 1998;80:129-32.
8. Chalian VA, Barnett MO. A new technique for constructing a one-piece hollow obturator after partial maxilllectomy. J Prosthet Dent 1972;28:448-53.
9. Wu Y, Schaaf NG. Comparison of weight reduction in different designs of solid and hollow obturator prostheses. J Prosthet Dent 1989;62:214-7.
10. Morrow RM, Rudd KD, Rhoads JE. Dental Laboratory Procedures; Complete dentures. Vol 1, 2nd ed. Mosby: St .Louis,1985.p.312-24.
|