Introduction
High levels of clinical success in endodontic treatment is through complete cleaning, shaping and obturating the canal space in three dimensions which require a thorough knowledge of root canal anatomy and morphology.[1],[2] While treating each tooth theclinician must assume that complex anatomy occurs often enough to be considered normal. Therefore, the unusual number of canals should always be expected in various teeth.[3]
Mandibular premolars have great variability in their internal morphology due to the presence of more than one root canal, lateral canals, fins etc which may complicate the cleaning procedures.[4] They are regarded as Endodontist’s enigma as they are unpredictable. Incomplete cleaning of all the irritants can result in persistent inflammation and failure of endodontic therapy.[5]
Ingle[6] has reported that the canal configuration might account for greater increase in endodontic failures of these teeth. Radiographs, computed tomography and optical microscopy can diagnose these morphologic variations of the pulp cavity. The role of genetics and racial variation may result in differences of incidence of root numbers and canal number in human population. Varella Jstudied the45 X-chromosome of females in Finland and found that X chromosomes have a gene or genes with a regulatory function in root development.[7]
Variation in the root canal system of mandibular premolars has been reported. Vertucci FJ[8] and Zillich and Dowson[9] reported the occurrence of 3 canals in mandibular second premolars to be 0.0% and 0.4% respectively. Vertucci using a transparent method found 25.5% of 400 mandibular premolars had two apical openings and 0.5% of the teeth had three apical openings.[10] Hulsmann[11] (1990) and El deeb[4] (1982) reported 3 canals in mandibular premolars. Recent clinical reports have described some infrequent cases of mandibular second premolars with four canals[12],[13],[14] or five canals.[15]
These reports show that although the incidence of occurrence of more root canals in mandibular second premolar is low but still such anatomic variations might occur in clinical practice.The aim of this article is to report an uncommon condition of mandibular second premolar with three distinct canals.
Case Report
A 38-year-old male patient reported to our clinic with pain in his lower right second premolar since few days. History of present illness revealed that the patient had experienced sensitivity to cold drinks since four months and reported pain for the past ten days. Pain was spontaneous in nature and aggravated in the night due to food impaction and was relieved on taking medication. Medical history was found to be non-contributory.
The intraoral clinical examination revealed carious # 45 and 46. Thermal tests showed immediate response in #45 and 46 while with electric pulp tester there was delayed response suggesting of irreversible pulpitis with absence of swelling or sinus tract in near vicinity.
On radiographic examination, the preoperative radiograph showed disto-occlusal radiolucency approximating the pulp chamber of 45 and mesio-occlusal radiolucency approaching mesial horn of 46. There was symmetrical widening of the periodontal ligament space. The periodontal ligament suggested an abnormal anatomical feature. Periapical radiograph revealed bifurcation at the level of middle third of root into mesial and distal root. The probable diagnosis was an acute irreversible pulpitis in # 45 and 46. So, the endodontic treatment was indicated in both the teeth.
The patient received local anesthesia (2% lidocaine with 1:100,000 adrenaline) and a rubber dam was placed. Caries was removed prior to access opening. Access was gained to the pulp chamber with round diamond bur in 45. After reaching the pulp chamber, the roof was removed and lateral walls were prepared with a safe-end tapered bur (Endo-Z; Dentsply) positioned parallel to the long axis of the tooth. Access was broadened mesio-distally to locate the canals. Mesial and distal canals were located with no.8 and 10 K files (Dentsply/Maillefer). During the canal preparation the initial instrument crossed when placed into the canals. Therefore the access cavity was widened in the lingual side where there was residual pulp chamber roof, suggesting the presence of a lingual canal. Exploration of the pulp chamber with DG 16 probe also confirmed the presence of three root canals: mesial, distobuccal and distolingual, suggesting of Type III distal canals (Weine’s classification).16 Examination of the pulp chamber floor with microscope also revealed three distinct orifices (Figure 1).
 | Figure 1 : Pulp Chamber With Three Canal Orifices.
 |
The canals were irrigated with 5.25% sodium hypochlorite and working length was determined using Endomaster and radiographically. Preflaring of the canals was done with Hyflex NiTi .08/25 for straight line access to all the three canals. Biomechanical preparation was done using Hyflex CM NiTi files with master apical file .04/25. The canals were irrigated with 5.25% NaOCl and then later obturated by lateral compaction of gutta percha cones and AH26 sealer (Dentsply) (Figure 2).
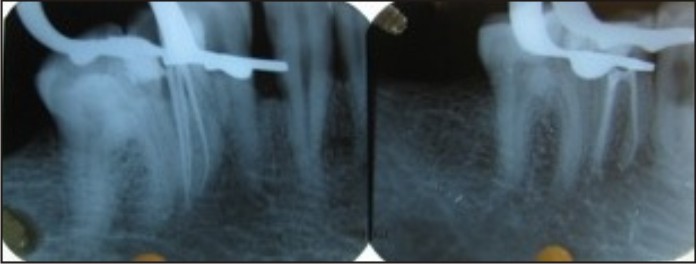 | Figure 2 : Mastercone Iopar And Iopar Showing Obturated Three Canals.
|
Discussion
The presence of extra roots or canals in mandibular premolars is undoubtedly an endodontic challenge. The clinician must be familiar with the various pathways root canals take to the apex. The pulp canal system is complex and canals may branch, divide and rejoin.
Mandibular second premolar usually has one root and one canal. However a second canal has been identified in up to a third of teeth, and three canals occasionally. Slowey[17] has suggested that the mandibular premolars may present the greatest difficulty of all teeth to perform successful endodontic treatment. A University of Washington studyassessed the failure rate of non surgical RCT in all teeth. It was highest for the mandibular premolars at 11.45%. The possible reasons for a high failure rate are the numerous variations in root canal morphology and difficult access to a second canal, potentially resulting in a missed canal.[6]
Careful interpretation of the periodontal ligament space may suggest the presence of an extra root or canal. Mesial and distal angled views often reveal the presence of a bi or trifurcation of the root. Careful evaluation of two or more periapical radiographs is mandatory. Using the ‘fast break’ guideline as stated by Nattress and Martin[18]. In the present case the preoperative radiographs made us suspicious of some anatomical complexity in the root canal system which was characterized by a complete mid root separation of the canals into mesial and distal. Although Bifurcation of roots among lower premolars usually occurs buccolingually but in this case the mesiodistal branching is quite significant and rare. The premolars being the transition tooth in the arch may be the reason for these variations simulating the molars.[19]
The access cavities in mandibular premolars are small but to visualise and locate the extra root canals in certain cases, we need to widen the access. The access cavity should have divergent walls to the occlusal surface. The pulp chamber that appears to be deviated from this normal configuration and seems to be either triangular in shape or too large in mesiodistal plane should be suspected of opening into a system containing three canals (Bellizi and Hartwell 1981).[20]
Although in vitro and in vivo studies[8],[9],[10],[11] report low incidence of mandibular second premolars with three canals but still careful interpretations of preoperative radiographs, the periodontal ligament space and the anatomical aspects of the pulp chamber roof helps to identifying the internal variations, thus facilitating the locations of all root canals.[17],[21]
In this case report some opening resistance was felt during the initial negotiation of the canals with no. 08 and 10 K files indicating the presence of more root canals. Both the tactile sensitivity and the observation of the direction of endodontic instrument during its introduction into the canal are important to locate all the canals. A DG16 endodontic probe used as pathfinder determines the angle at which the canals depart from the main chamber.[22]
Preflaring of the cervical portion of the canal allowed a correct working length determination and better cleaning of the apical third and filling of the root canals. The crown-down approach was used in the present case until the desired length was reached. This technique had the advantage of enlarging and cleaning the coronal area before proceeding deeply into the apical regionsfrom where majority of the infected tissue was removed (Marshall & Pappin 1980).[23] Furthermore, it provided unobstructed access for instruments to follow. This also helped to minimize post-operative discomfort by preventing the inoculation of periradicular tissues with bacteria and necrotic tissue that might be pushed out by hand files.[5]
Thorough knowledge of the possible aberrations in the pulp canal spaces of teeth prior to the treatment can help the dentist realize and manage the root canal system in a better way.
Conclusion
The clinician should have an accurate knowledge about the anatomy of each tooth as well as the possibility of variations, to identify the presence of unusual numbers of roots and their morphology. This may help to reduce endodontic failure caused by incomplete obturation. Careful interpretation of the radiograph, close clinical inspection of the floor of the chamber and proper modification of access opening are essential for a successful treatment outcome.
References
1. Tzu-Yi Lu, Shue-Fen Yang and Sheng-Fang Pai. Complicated Root Canal Morphology of Mandibular First Premolar in a Chinese Population Using the Cross Section Method. J Endod 2006;32:932–936
2. Gomes FA, Carvalho de Sousa B, Santos RA. Unusual anatomy of mandibular premolars. Aust Endod J 2006;32:43-5.
3. Walton RE, Vertucci FJ (1996) Principles and Practice of Endodontics, 2nd edn. Philadelphia, PA: W.B. Saunders Co.
4. ElDeeb M: Three root canals in mandibular secondpremolars. Literature review and case report. Journalof Endodontic, 1982; 8:376-377.
5. S Tyagi, KP Arjun Das & SV Bhagwat. Endodontic enigma – Mandibular second premolar with Three Root Canals: A Case Report. People’s Journal of Scientific Research.2008; 1: 27-29
6. Ingle J, Bakland I. Endodontics. 5th ed. Hamilton: BC Decker; 2002.
7. Varella J. Root morphology of mandibular premolars in human 45,X females. Arch Oral Biol 1990; 35 : 109-12.
8. Vertucci F. Root canal morphology of mandibular premolars. J Am Dent Assoc1978;97:47–50.
9. Zillich R, Dowson J. Root canal morphology of mandibular first and second premolars.Oral Surg Oral Med Oral Pathol 1973;36:738–44.
10. Vertucci FJ. Root canal anatomy of the humanpermanent teeth. Oral Surg Oral Med Oral Pathol1984;58:589-99
11. Hulsmann, M.: Mandibular first premolar with three root canals. Endo. Dent. Traumatol. :6, 189,1990.
12. Wong M. Four root canals in a mandibular second premolar. J Endod 1991;17:125– 6.
13. Holtzman L. Root canal treatment of mandibular second premolar with four rootcanals: a case report. Int Endod J 1998;31:364–6.
14. Al-Fouzan KS. The microscopic diagnosis and treatment of a mandibular secondpremolar with four canals. Int Endod J 2001;34:406 –10.
15. Macri E, Zmener O. Five canals in a mandibular second premolar. J Endod2000;26:304 –5.
16. Weine FS. Endodontic therapy. 6th edition, St.Louis,1996, Mosby, p 243.
17. Slowey RR Root canal anatomy. Road map to successful endodontics. Dent Clin North Am 1979;23:555–73.
18. Nattress BR, Martin DM. Predictability of radiographic diagnosis of variations in root canal anatomy in mandibular incisor and premolar teeth. Int Endod J 1991;24:58-62.
19. Iyer VH, Indira R, Ramachandran S, Srinivasan MR. Anatomical variations of mandibular premolars in Chennai population. Indian J Dent Res 2006; 17 : 7-10.
20. Bellizzi R, Hartwell G. Evaluating the maxillary premolar with three canals for endodontic therapy. Journal of Endodontics 1981; 7: 521-7.
21. England MC Jr, Hartwell GR, Lance JR. Detection and treatment of multiple canals in mandibular premolars. J Endod 1991, 17; 174-178.
22. Burns RC, Herbranson EJ. Tooth morphology and access cavity preparation. Cohen S, Burns RC, eds. Pathways of pulp. 8th ed. St. Louis, MO: Elsevier Mosby; 2002. P.181.
23. Marshall F, Pappin J: A crown-down pressurelesspreparation root canal enlargement technique. InTechnique manual. Oregon Health & SciencesUniversity, Portland, Oregon, 1980.
|