Introduction
Dental caries has historically been considered a significant global oral health burden and international data on caries epidemiology confirms that tooth decay is not only a significant disease of childhood but prevalence of dental caries is high among adults also.[1],[2] It is important to target prevention of dental decay from an early age since it is a chronic irreversible process that once occurs, persists throughout life even though the lesion is treated.[2],[3],[4] It is notable that the prevalence of dental caries among children and adults is approximately 60–65% in India.[5],[6],[7],[8],[9]
In Punjab, majority population resides in the rural sector (62.52%), with a total population of 2.77 Crore, however, non-accessibility and non-affordability of dental facilities continues to be the foremost problem in rural areas of Punjab.[10],[11] Currently, dental professionals in India have accessibility to the most recent advances in dental treatment and materials. Additionally, there are 289 dental institutions in total, generating more than 30,000 dental graduates each year. Nonetheless, dental caries continuous to be a major public health issue in rural areas of India, with the current dentist to population ratio being 1:2,50000 as compared to 1:10,000 in urban areas.[12] Moreover, not only is the baseline data on prevalence of dental diseases among children in Punjab scarce, there is no published literature available on the dental status of adults in Punjab from the last three decades. Hence, the aim of our study was to assess the oral health status and corresponding treatment needs in the rural population of Ferozepur District of Punjab.
Methodology
A descriptive cross-sectional study was conducted among the rural population of the following villages of Ferozepur District of Punjab: Malwala, Kadim and Bajidpur. Places of worship and various community centres of the villages were selected as the sites for survey. Participation in the study was voluntary and an informed consent was obtained from the parents for subjects that were below 18 years of age. Information regarding demographics and oral health status was collected via questionnaire and clinical examination. World Health Organization (WHO) Oral health Assessment Form (1997) was used to assess dental caries prevalence and treatment needs.[13] Also, all subjects participating in the study were provided free dental treatment. Dental status and demographic details were noted on standardized format data sheets, which were then transferred to a computer for analysis and review. Both non-parametric and parametric tests were applied to analyse the results. We used an alpha level of .05 for all statistical tests.
Results
A total of 340 subjects between the age groups of 12 to 74 years were clinically examined regarding their oral health status and treatment need. The study population consisted of both sexes with 55.9% (n=190) females and of the total sample, 24.7% (n=84) were 12-year olds (Table I).
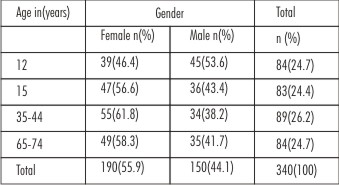 | Table I - Distribution Of Sample By Age And Gender
 |
Evaluation of oral health status of the study population revealed that dental caries is the most prevalent disease across all age groups. The prevalence of Decayed, Missing and Filled Teeth (DMFT) by age is given in (Table II). A Chi-square test of independence was performed to examine the relation between gender and dental decay. The relation between these variables was significant (c2= 5.38, P<0.01). Dental decay was found to occur in 67.94% (n=231) of the total population and males were less likely to have decayed teeth (39.81%, n=92) as compared to females (60.17%, n=139). Also, females were significantly more likely to have atleast one decayed, missing or filled tooth (DMFT=1) as compared to males (c2= 4.65, P<0.02).
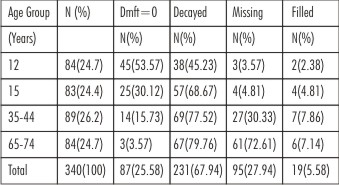 | Table II - Prevalence Of Decayed, Missing And Filled Teeth By Age
|
A one-way between subjects Analysis of Variance (ANOVA) was conducted to compare the effect of age on dental caries prevalence in all four age groups. There was a significant effect of age on dental caries prevalence at the p<0.05 level for the four age groups (F (3,336) = 17.92, P<0.001). Post hoc comparisons using the Tukey HSD test indicated that the mean score for the 12-year-old subjects (M = 1.37, SD = 2.43) was significantly different than that in the 35-44 years (M = 3.89, SD = 3.60) and 65-74 years age groups (M = 5.21, SD = 3.96). However, the 12 year olds did not significantly differ from the 15 year olds (M=2.28, SD = 2.94). Mean score for dental caries in the 15-year-olds was significantly different than that in the 35-44 years and 65-74 year old age groups also. Specifically, our results suggest that when the sample population increases in age, there is an increase in the mean number of decayed teeth in the subjects. However, it should be noted that there must be a sizeable age difference between the groups in order to see an effect.
It is noteworthy that only 25.58% (n=87) of the sample had no decayed, missing or filled teeth (DMFT=0) and the filled component was almost negligible (5.58%, n=19). Also, 30.3% (n=103) of the sample had a mean DMFT ranging from one to three while 44.1% (n=150) had a mean DMFT value of four or more. The overall mean DMFT of the sample was observed to be 5.81±7.80 with the mean DMFT ranging from 1.45±2.51 in the 12 year olds to 13.81±7.80 in the age group of 65-74 years due to the presence of edentulous subjects in the older age group (Table III). Additionally, in a total of 231 subjects with dental caries, 1072 teeth were found to be carious. The most affected teeth by dental caries were the first and second molars and made up for more than half of the total number of decayed teeth (53.4%, n=463). Overall teeth in the mandibular arch (51.6%, n=448) were more affected as compared to the maxillary arch (48.3%, n=419) (Table IV).
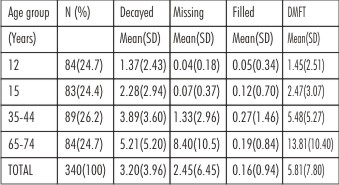 | Table III - Distribution Of Dental Status And Mean Dmft By Age
|
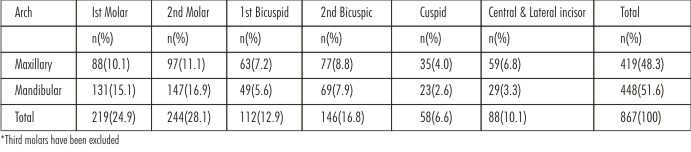 | Table IV - Distribution Of Number Of Decayed Teeth By Tooth Type
|
Oral health examination showed that a total of 95.88% (n=326) subjects required dental treatment and out of those needing treatment, 83% required atleast three treatment items (Table V). Grossly decayed and damaged teeth with poor prognosis were considered as those recommended for extraction. Out of a total of 67.94% (n=231) subjects that had dental caries, 18.18% (n=42) required tooth extraction. Gross dental decay was found to be more prevalent in the age group of 35-44years and 65-74 years. One-surface filling was the maximum treatment need followed by the need for a crown with a total of 61.17% (n=208) and 19.7% (n=67) subjects requiring it respectively. Pulp treatment was required by only 2% (n=7) of the subjects and this could be due to no radiological examinations being done. It was interesting to note that the need for RPD/Implants was high (14.4%(n=49) and majority Crowns were needed in the 65-74 yrs old age group (n=40).
Regarding the prosthetic status, 14% (n=49) subjects required some form of prosthetic treatment in the upper arch as compared to a 17.94%(n=61) need in the lower arch. A one unit prosthesis was required by 4.70% (n=16) and 5.90% (n=20) subjects in the upper and lower arches respectively. There was also a need for multi unit prostheses by 4.10% (n=14) and 6.8% (n=23) subjects in the upper and lower arches respectively and 5.29% (n=18) of the subjects needed complete dentures.
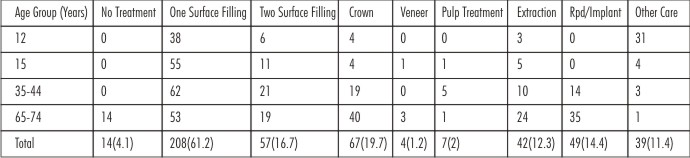 | Table V - Distribution Of Treatment Need By Age Group
|
One–surface filling was needed by 61.5% (n=128) females as compared to only 38.5% (n=80) males and this difference was significant (c2=6.95, P<0.006). All those subjects requiring any other treatment such as: full mouth rehabilitation; extraction of retained primary teeth; treatment of dental anomalies; bleaching; and pit and fissure sealants, were recorded as those needing other care. There was also a significant difference found by gender in subjects needing other care (c2=3.94, P<0.03) (Table VI).
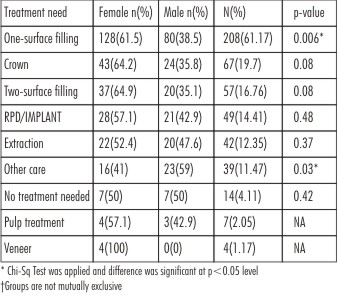 | Table VI - Distribution Of Treatment Need By Gender
|
Discussion
Various studies conducted in India illustrate that decayed teeth account for the highest percentage of DMFT as was observed in our study sample.[10],[14],[15],[16] The overall dental caries prevalence of 67.94% and mean DMFT of 5.8±7.80 in our sample shows that dental decay is still among the major dental problems affecting the rural population of Punjab. Our results were comparable to those reported by studies conducted in other areas of North India. Kaur R.[11], reported similar caries prevalence of 63.20% on a study among 16 to 21 years olds in Punjab. Analogous results were also reported in a study in Rajasthan among 15 to 54 year olds whereby the mean DMFT was observed to be 5.34.[17] Maru AM.[7], in a study on rural population of Gujarat between the age group of 20 to 60 years observed the caries prevalence to be 80% and a mean DMFT of 5.1.
However, higher caries prevalence as compared to our study (67.94%) has also been reported in a recent study among 12 and 15 year old school children residing in Ludhiana (Punjab) whereby the caries prevalence was observed to be 81.36% and 86.16% respectively.[10] Kalra S.[18] also observed a higher caries prevalence of 83% among 12 to 13 year old school children in Haryana. The authors attributed high caries prevalence to poor oral hygiene and overall negligence of oral health. On the other hand, studies conducted in Faridkot District of Punjab have reported a lower caries experience, analogous to our study, than that observed by other studies in Punjab.[19],[20] One of the reasons for this variation could be due to both Faridkot and Ferozepur being situated in the high fluoride belt region of Punjab. Additionally, caries rate in our study showed an increase with age and research shows that caries rates in the permanent dentition are expected to increase with age probably due to prolonged exposure of teeth to caries associated risk factors.[5],[8]
A review of gender variation in dental decay illustrated that females showed higher caries prevalence than males in the present study, similar to that observed by other authors in India.[8],[21] Khan AA.[22] in a study conducted in Gwalior on 11 to 80 year olds also observed that females had a higher caries prevalence rate (51.41%) than males (49.51%). It is postulated that the observed variation in caries prevalence rates in the documented data could have been due to differences in: oral hygiene practices, accessibility to dental health care facilities, diet or a variation in research methodology.
Another noteworthy trend was the presence of higher decay among the first and second molars and higher prevalence of decay in the mandibular arch. Chawla HS.[23], Saravanan S.[24] and Udoye C.[25] also observed similar trends. Furthermore, the overall high treatment need and lack of restorations, suggests that there is a high prevalence of dental caries and lack of dental care in the rural areas and this is in accordance with similar studies conducted elsewhere. In our study, need for one surface filling (61.20%) was the maximum in all groups, followed by the need for a crown (19.70%) and two surface fillings (16.70%). Maru AM.[7] reported comparable results in a rural population of 20 to 60 year olds in Gujarat whereby he observed that the need for one surface filling, two surface filling, crown and extraction was 60.80%, 16.90%, 23.80% and 37.60% respectively. Mandal KP.[6], in a study conducted in East India, found that in the age group of 5 to 35 years, the need for single surface restorations was maximum; indicating lack of restorative treatment, preventive oral care facility, and awareness among population.
The need for tooth extraction in our study was 12.3% and showed an increase with age. Our results were comparable to those reported by Saravanan S[5] in a study conducted on school children in Tamil Nadu wherein almost 3% to 15% of the children in his study needed extraction. The need for extraction in our sample was lower than that observed by Munjal V[10], which was 15.41% in 12 year olds, and this again could be due to lower caries experience found in our study due to Ferozepur being in the high Fluoride belt region of Punjab.
Conclusion
Our study provides a comprehensive review of oral health status and existing treatment needs among the rural population of Punjab. Clearly, it can be established that this community has experienced a low utilization of oral health services mainly due to the lack of dental facilities in rural areas of Punjab owing to the disproportionate distribution of dental professionals in urban and rural India. The need for dental health education including proper instruction of oral hygiene practices and school based preventive programs is vital as they would be beneficial for a lifetime. Lastly, there is a need to integrate the existing oral health care infrastructure with the rural community health centres to ensure that oral health problems identified through dental surveys are treated in a timely manner.
References
1. Petersen PE, Bourgeois D, Ogawa H, Estupinan-Day S, Ndiyae C. The global burden of oral diseases and risks to oral health. Bulletin of the World Health Organization. 2005;83:661–669.
2. Selwitz RH, Ismail AI, Pitts NB. Dental caries. Lancet. 2007;369:51–59. doi: 10.1016/S0140-6736(07)60031-2.
3. Loesche WJ. Microbiology of Dental Decay and Periodontal Disease. In: Baron S, editor. Medical Microbiology. 4th edition. Galveston (TX): University of Texas Medical Branch at Galveston; 1996. Chapter 99. Available from: http://www.ncbi.nlm.nih.gov/books/NBK8259/
4. Ramachandran K, Rajan BP, Shanmungan S. Epidemiological studies of dental disorders in Tamil Nadu population, prevalence of dental caries and periodontal diseases. J Indian Dent Assoc. 1973;45:65–70.
5. Dhar V, Jain A, Van Dyke TE, Kohli A. Prevalence of dental caries and treatment needs in the school-going children of rural areas in Udaipur district. J Indian Soc Pedod Prev Dent. 2007;25:119–121.
6. Saravanan S, Kalyani V, Vijayarani MP et al. Caries prevalence and treatment needs of rural school children in Chidambaram Taluk, Tamil Nadu, South India. Ind J Dent Res. 2008;19:186-90.
7. Mandal KP, Tewari A, Chawla HS, Gauba K. Prevalence and severity of dental caries and treatment needs among population in the Eastern states of India. J Indian Soc Pedod Prev Dent. 2001;19:85-91.
8. Maru Am, Narendran S. Epidemiology of dental caries among adults of rural areas of India. J of Contemp Dent Pract. 2012;13(3):382-388.
9. J. David, Wang NJ, Astrom AN et al. Dental caries and associated factors in 12-year-old school children in Thiruvanathipuram, Kerela, India. Int J Paed Dent. 2005;15(6):420-8.
10. Facts about states of India Population Census 2011. India. Available from: http://www.census2011.co.in/facts/state.php
11. Family Welfare statistics in India 2011. Ministry of Health & Family Welfare. India. Avaliable from: https://nrhm-mis.nic.in/familywelfare2011.html
12. Munjal V, Gupta A, Kaur P et al. Dental caries prevalence and treatment needs in 12 and 15-year-old school children of Ludhiana city. Ind J Or Sci. 2013;4(1):27-30.
13. R Kaur, H Kataria, S Kumar et al. Caries Experience among Females aged 16–21 in Punjab, India and its Relationship with Lifestyle and Salivary HSP70 Levels. Eur J Dent. 2010;4(l3):308–313.
14. Ahuja NK , Parmar R. Indian Journal of Dental Sciences. Demographics & Current Scenario with respect to Dentists, Dental Institutions & Dental Practices in India. 2011 June;2(3):8-11.
15. World Health Organization (1997). Oral health Surveys-Basic Methods. 4th ed. Geneva. World Health Organization.
16. Singh AA, Singh B, Kharbanda OP et al. A study of dental caries in school children from rural Haryana. J Ind Soc Pedodont Prev Dent. 1999;17(1):24-8.
17. Grewal H, Verma M and Kumar A. Prevalence of dental caries and treatment needs in the rural child population of Nainital District, Uttaranchal. J Ind Soc Pedodont Prev Dent. 2009; 27(4):224-6.
18. Bhowate RR, Borle SR, Chinchkhede DH et al. Dental R32;health amongst 11–15 year-old children in Sevagram Maharashtra.R32;Ind J Dent Res. 1994;5(2):65–8.
19. Kumar TS, Dagli RJ, Mathur A, Jain M, Balasubramanyam G, Prabu D, Kulkarni S. Oral health status and practices of dentate Bhil adult tribes of southern Rajasthan, India. Int Dent J. 2009 Jun;59(3):133-40.
20. Kalra S, Simratvir M, Kalra R, Janjua K, Singh G. Change in dental caries status over 2 years in children of Panchkula, Haryana: A longitudinal study. J Int Soc Prevent Communit Dent. 2011;1:57-9
21. Singh S, Kaur G, Kapilla VK. Dental disorders in primary school children of Faridkot city. J Indian Dent Assoc. 1985;57:304-8.
22. Singh N, Goyal V, Kaur S, Bhola M, Gupta P. Prevalence of dental caries among children with special health care needs in Ludhiana and Faridkot Districts of Punjab. Baba Farid Univ Dent J. 2013;4(1);1-5.
23. Rajaratnam J, Devi S, Asirvatham M et al. Prevalence and factors R32;influencing Dental problems in a rural population of southern India. Tropical Doctor. 1995; 25(3):99–100.
24. Khan AA, Jain SK, Shrivastava A. Prevalence of Dental Caries among the Population of Gwalior (India) in Relation of Different Associated Factors. Eur J Dent. 2008 Apr;2:81-85.
25. Chawla HS, Gauba K, Goyal A. Trend of dental caries in children of Chandigarh over the last sixteen years. J Indian Soc Pedod Prev Dent. 2000;18(41);5-12.
26. Saravanan S, Madivanan I, Subashini B, Felix J W. Prevalence pattern of dental caries in the primary dentition among school children. Indian J Dent Res. 2005;16:140
27. C Udoye, E Aguwa, R Chikezie, M Ezeokenwa, O Jerry-Oji, C Okpaji. Prevalence and distribution of caries in the 12-15 year urban school children in Enugu, Nigeria. The Internet Journal of Dental Science. 2008;7(2).
|