Introduction
Over the years pain and discomfort have been the major causes for which patients have sought unscheduled or emergency dental visits. With the evolution of dentistry, these causes have largely been eliminated. As a consequence of the new age lifestyle in the 21st century, new afflictions have arisen.
Dentinal hypersensitivity is a frequent problem, most commonly, affecting the facial surface of premolars and canines[1]. It afflicts perhaps 15% of the adult population throughout and possibly upto 57% in some regions[2]. The international workshop held at Newark, NJ, USA in November 1994 defined dentinal hypersensitivity as[3]: “A short, sharp pain arising from exposed dentinal in response to stimuli, typically thermal, evaporative, tactile, osmotic or chemical and which cannot be ascribed to any other dental defect or pathology”. The Canadian Advisory Board in the year 2003 suggested a modification of the present definition[4] in which they substituted ‘disease’ for ‘pathology’.
Various theories have been put forth to explain the actual mechanism of dentinal hypersensitivity. The hydrodynamic theory given by Brännström in the year 1964 is the most accepted theory.[2]
The desired goal for treatment of dentin hypersensitivity is attainment of immediate and lasting relief from discomfort. This can be accomplished either by a passive mechanism such as precipitation of salivary calcium phosphate inside the dentinal tubules and the adsorption of plasma protein or by an active mechanism which uses desensitizing agent alone or as an adjunct to another dental procedure[5].
The present in vitro study was conducted to evaluate the efficacy of diode laser and desensitizing pastes containing Pro-Argin, Hydroxyapatite and Novamin respectively in occluding the dentinal tubules over a period of 7 days using Scanning electron microscopy.
Material And Method
A total of 25 dentin blocks were obtained from the roots of the single rooted teeth and stored in saline. All experiments were conducted within 1 month of extraction.
Inclusion Criteria
1. Periodontally compromised single rooted anterior teeth within one month of their extraction.
2. Caries free root surface.
3. Roots without any wasting disease (Abrasion, Erosion, Abfraction)
Fractured roots, endodontically treated teeth and prosthodontically restored teeth were excluded.
Preparation Of The Samples
The diseased root surfaces of all teeth were firstly scaled with an ultrasonic scaler. Samples were taken from the root by marking four parallel grooves with a tapered diamond bur in a micromotor hand-piece under copious saline irrigation. The grooves were positioned horizontally at CEJ and at 3 mm, 6mm and 9mm away from the CEJ (Fig1). With the help of a diamond disc the six blocks were obtained firstly by transversely sectioning the root from the grooves and secondly by dividing the sample longitudinally into two from the middle (Fig 1). The labial and lingual surface of each specimen was used for the study[6]. Dentine segments were polished using a 500 grit abrasive paper to compose a flat dentin and smear layer. The smear layer was then removed by ‘active burnishing’ for three minutes with citric acid at pH-1. The cotton pellets were changed every 30 seconds to ensure consistent solution application[6].
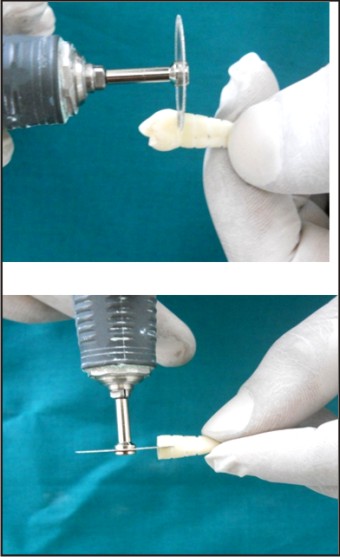 | Fig 1 : Preparation Of Dentin Blocks
 |
Subsequently the sections were copiously rinsed with deionized water for a period of 30 seconds and air dried. The sections were randomly divided into five groups:
Group A – Calcium Sodium Phosphosilicate
Group B- Pro-Argin
Group C- Diode Laser (940nm)
Group D- Hydroxyapatite
Group E- Control.
The agents for groups A, B and D were applied using an applicator brush for a period of 2 minutes twice daily. The dentin blocks in group C were irradiated with diode laser (940nm) with the following parameters: 0.5 W in PW (T on 100ms and T off 100ms) and fluence of 62.2 J/cm2 in no contact mode. Each site received 3 applications of 1 min each[7] (Fig 2). The samples were stored in artificial saliva at 37I0; C at a pH of 7 for a period of seven days under a continuous stirring (100rpm). The composition of the artificial saliva was similar to the human saliva and was prepared using the following reagents: 1.09mmol/LCaCl2, 0.68mmol/LKH2PO4, 30mmol/L KCl, 2.6µmol/L NaF and 50mmol/L HEPES. The HEPES was used to buffer the pH of the saliva at 7.0, this was checked using the pH meter[8]
Each segment was treated with their respective agents every day for the next seven days. The synthetic saliva was replenished every 6 hours to minimize change in ion concentration, simulating conditions in the oral environment[8].
The samples were dehydrated in a graded series of ethanol (10%, 20%, 30%, 40%, 50%, 60%, 70%, 80%, 90%) for 1 hour each and 100% ethanol for a period of 1 hour. After the chemical treatment all the samples were dried under the lamp for approximately 30 minutes. The flat pulpal surface of samples was mounted on the aluminium stubs with a double sided adhesive tape with the outer surface (buccal/lingual) facing the beam of the SEM (Leo -430). Gold palladium coating was done on each mounted specimen in a Polaron – SC7640 Sputter Coater machine. The coated samples were examined at a magnification of 5000X by SEM at regular intervals of 0, 24, 72, 120 and 168 hours[8]. The photomicrographs were analysed by three blind, trained examiners to assess the percentage (%) of tubular occlusion. The percentage of occluded tubules was calculated by using the following equation[9]
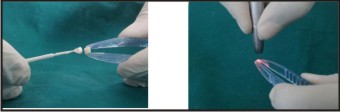 | Fig 2 : Application Of Agents : Dentifrice And Diode Laser
|
%OCT =
number of occluded tubules x 100
-----------------------------------------
Total number of tubules
This percentage represents the occlusion exhibited by the different treatments used and also showed the occlusion relative to the maximum number of open tubules obtained after citric acid.
Results
The results of the present study are summarized inpercent change from 0 to 168 hours. The z test has been used as a test of significance. The results were statistically significant (p=0.01) for percentage of tubular occlusion after72 and 168 hours for all the test groups. The z test has been used as a test of significance.
The percentage of occluded tubules increased significantly (p=0.01) from 0 hours to 24, 72, 120 and 168 hours in all the groups (Table 1). A significant (p<0.0001) difference was observed between group E and all the groups- A, B, C and D at 0, 24, 72,120 and 168 hours.
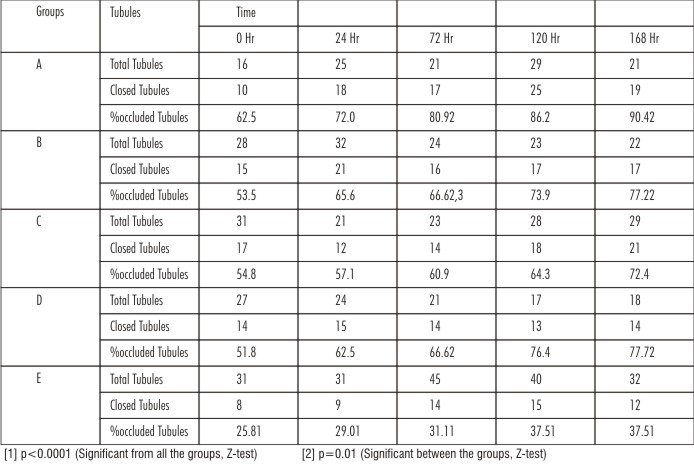 | Table-1: Comparative Evaluation Of The Percentage Of Tubular Occlusion Among All The Groups And Follow-ups.
|
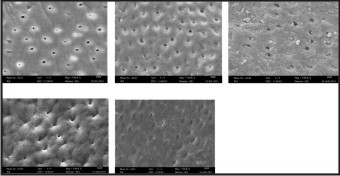
The dentin blocks in Group A were subjected to treatment with CSPS. The results of the scanning electron microscopic study revealed that it was able to occlude 62.5%, 72%, 80.9%, 86.2% and 90.4% of the dentinal tubules at 0, 24, 72, 120 and 168 hours after immersion in artificial saliva (Fig 3). There was a statistically significant increase in the percentage of tubular occlusion (p=0.01) from 0 to 24, 72, 120 and 168 hours. (Table.1).
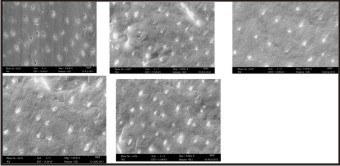 | Fig 3 : SEM At 5000x For Calcium Sodium Phosphosilicate At 0,24,72,120 & 168 Hours
|
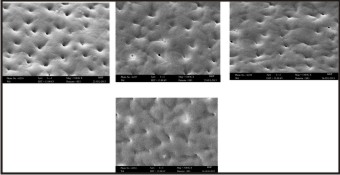
The dentin blocks in Group B were subjected to treatment with PA. The results of the scanning electron microscopic study revealed that it was able to occlude 53.5%, 65.6%, 66.6%, 73.9% and 77.2% of the dentinal tubules at 0, 24, 72, 120 and 168 hours after immersion in artificial saliva. (Fig 4) There was a statistically significant increase in the percentage of tubular occlusion (p=0.01) from 0 to 24, 72, 120 and 16 hours. (Table 1).
 | Fig 4 : SEM At 5000x For Pro-argin At 0,24,72,120 & 168 Hours
|
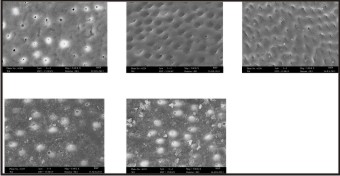
The dentin blocks in Group C were subjected to treatment with DL. The results of the scanning electron microscopic study revealed that it was able to occlude 54.8%, 57.1%, 60.9%, 64.3% and 72.4%of the dentinal tubules at 0, 24, 72, 120 and 168 hours after immersion in artificial saliva (Fig 5). There was a statistically significant increase in the percentage of tubular occlusion (p=0.01) from 0 to 24, 72, 120 and 16 hours. (Table 1).
 | Fig 5 : SEM At 5000x For Diode Laser At 0,24,72,120 & 168 Hours
|
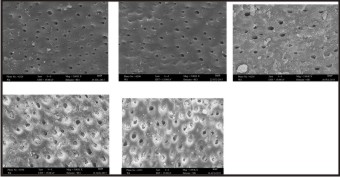
The dentin blocks in Group D were subjected to treatment with HA. The results of the scanning electron microscopic study revealed that it was able to occlude 62.5%, 72%, 80.9%, 86.2% and 90.4% of the dentinal tubules at 0, 24, 72, 120 and 168 hours after immersion in artificial saliva (Fig 6). There was a statistically significant increase in the percentage of tubular occlusion (p=0.01) from 0 to 24, 72, 120 and 168 hours. (Table.1)
 | Fig 6 : SEM At 5000x For Hydroxyapatite At 0,24,72,120 & 168 Hours
|
The dentin blocks in Group E were not subjected to any active form of treatment (Control). The results of the scanning electron microscopic study revealed that the percentage of tubular occlusion was 25.8%, 29%, 31.1%, 37.5% and 37.7% at 0, 24, 72, 120 and 168 hours after immersion in artificial saliva. (Fig 7).
 | Fig 7 : SEM At 5000x For Control At 0,24,72,120 & 168 Hours
|
Discussion
Dentine hypersensitivity (DH) is a painful response of the tooth to different stimuli such as brushing, low pH beverages, occlusal overload, dental caries and thermal changes[10]. DH is characterized by a rapid onset of sharp burst of pain, lasting for seconds or minutes. The desired goal for treatment of dentin hypersensitivity is attainment of immediate as well as lasting relief from discomfort. This is achieved by application of a desensitizing agent used alone or as an adjunct to another dental procedure. Till date no such treatment has been discovered and there is no ‘gold standard’ by which one can assess the efficacy of the agent used[11].
Since dentinal hypersensitivity can recur over time even in the same individual one must be able to decisively diagnose and recognize the predisposing factors to formulate a treatment plan for effectively managing dentinal hypersensitivity. The goal of the present study was to find out the most efficacious agent amongst Diode Laser (DL), Calcium Sodium Phosphosilicate (CSPS), Pro-Argin (PA) and Hydroxyapatite (HA) in occluding dentinal tubules.
A statistically significant increase in the percentage of tubular occlusion (p=0.01) from 0 to 24, 72, 120 and 168 hours was seen in the dentinal blocks treated with CSPS (Table1). Similar results were observed by Burwell et al (2010)[12], who demonstrated that CSPS has the ability to rapidly occlude the dentinal tubules and releases calcium continuously to maintain the occlusion of the dentinal tubules.Furthermore, Earl et al (2011)[13] revealed that CSPS when applied on the dentin surface transforms from an amorphous material to a crystalline hydroxyapatite like material which helps in occluding the dentinal tubules. The findings of our study are in agreement with the above mentioned study. Another in vitro study by Wang et al (2010)[14] also revealed that CSPS containing desensitizing paste was highly effective in occluding the dentinal tubules. Gilliam et al (2002)[15] and Forsback et al (2004)[16] also revealed that dentifrice containing CSPS was superior in its action as compared to other agents.
Pro-Argin showed a statistically significant increase in the percentage of tubular occlusion (p=0.01) from 0 to 24, 72, 120 and 16 hours (Table1). These findings are in accordance with Irene Petrou et al(2009)[17] & Ahu Uraz et al (2013)[18], who noticed that the paste containing PA was highly effective in occluding the dentinal tubules by forming a plug and showed that it also penetrated into the dentinal tubules.
In dentin blocks treated with DL a statistically significant increase in the percentage of tubular occlusion (p=0.01) from 0 to 24, 72, 120 and 16 hours was reported (Table1). This finding is in accordance with Romeo et al (2012)[7] who stated that the DL acts by provoking a melting effect with the crystallization of the dentin inorganic matter and the coagulation of the fluid present within the dentinal tubules. However, in contrast Kimura et al (2000)[19] & Goharkhay et al (2007)[20], stated that the DL does not affect the surface of enamel or dentin morphologically and mediates only an analgesic effect. This difference in the result of our study can be accredited to the usage of a high power output DL which acts by melting the dentin thereby causing a tubular occlusion[23].
HA showed a statistically significant increase in the percentage of tubular occlusion (p=0.01) from 0 to 24, 72, 120 and 16 hours (Table1). Studies carried out by Ishikawa et al (1994)[21] and Suge et al (1995)[8] revealed that HA was able to occlude the dentinal tubules when viewed under SEM. Furthermore, Akatsura et al(2012)[22] revealed that the HAP particles were successfully deposited onto the dentin and solidified into the dentinal tubules. The results of our study coincide with the above mentioned study when evaluated sing SEM however in our study HA was applied utilizing an applicator brush.
The increase in the number of occluded tubules in Control group was because of the passive mechanism of tubular occlusion such as precipitation of calcium phosphate inside the tubules, adsorption of plasma proteins and saliva constituents as stated by Thereza et al (2004)[5].
Till date only a few studies have been conducted to compare the efficacy of the agents that were used in our study. The present in vitro study revealed Group A showed statistically significant (p=0.01) amount of dentinal tubular occlusion as compared to Groups B, C, D and E over the entire duration of the study. (Table 1) However contrary to our results, Salvatore et al (2010)[23] found that the occlusion of dentinal tubules by CSPS and PA did not have any statistically significant difference in their efficacy. This variation in the result can be explained with the difference in the parameters and methodology used in the respective studies.
There was no statistically significant difference between the Groups B, C and D at 0, 24,72 and 168 hours when analysed using SEM though Groups B & D showed a statistically significant difference at 120 hours (p=0.01) as compared to Group C (Table 1). The difference in the results can be attributed to difference in the mechanism of action of the agents and also due to the variation in the application.
Recently, studies have been performed to evaluate the efficacy of combining two or more desensitizing agents with that of the agent alone. An in vitro SEM study by Saeed et al(2013)[24] revealed that the effectiveness of combining hydoxyapatite and laser was superior to the other treatment modalities in sealing the dentinal tubules following a single application. As we did not use combination therapy we were not able to correlate this result to that of our study.
Conclusion:
Severity of dentinal hypersensitivity can be episodic. Hence establishing a concrete diagnosis becomes imperative in the attempts to identify and isolate an effective therapeutic agent for the elimination of Dentinal Hypersensitivity. In the current study all the experimental agents demonstrated an efficacy in occluding dentinal tubules as compared to the control group. The percentage (%) of occluded tubules was found to be highest for Calcium Sodium Phosphosilicate as compared to the other groups over a period of 7 days. However further long term studies are needed to critically warrant the usage of these agents.
References
1. D.G. Gilliam, R.Ochardson. Advances in the treatment of root dentin sensitivity: mechanisms and treatment principles. Endodontic Topics 2006;13:13-33.
2. Nicola X. West. Dentine hypersensitivity: preventive and therapeutic approaches to treatment. Periodontology 2000, 2008;48:31-41.
3. G.R Holland, M.N. Nahri, M. Addy, L. Gangarosa, R. Orchardson. Guidelines for the design and conduct of clinical trials on dentin hypersensitivity. Journal Of Clin Periodontol 1997;24:808-813.
4. Canadian Advisory Board on Dentin Hypersensitivity. Consensus-Based recommendations for diagnosis and management of dentin hypersensitivity. J Can Dent Assoc. 2003:69(4):221-226.
5. Thereza L, Antonio P, Roberto C, Pedro. A, Aldo J, Luc Louis W et al. Laser therapy in the treatment of dentin hypersensitivity. Braz Dent J 2004; 15(2): 144-150.
6. Sampaio JEC, Theodoro LH, Correa MA, Mendes AJD. A comparative SEM study of smear layer removal by detergents and EDTA on the root surfaces. Int J Periodontics Restorative Dent 2005; 25: 157-163.
7. Romeo U, Russo C, Palai G, Tenore G, Del V.A. Treatment of dentine hypersensitivity by diode laser : A clinical study. International Journal of Dentistry 2012; 1-8.
8. Suge T, Ishikawa K, Kawasaki A, Yoshiyam M, Asaoka K, Ebisu S. Duration of dentinal tubule occlusion formed by calcium phosphate precipitation method: in vitro evaluation using synthetic saliva. J Dent Res 1995; 74(10): 1708-1714.
9. Salvatore S,Timothy FW, Ian T, Dentin desensitization induced by prophylactic and air-polishing procedures: An in vitro dentin permeability and confocal microscopy study. Journal of Dentistry 2010; 38: 411-422.
10. Addy M, Urguhart E. Dentine hypersensitivity: its prevalence, aetiology and clinical management. Dent Update 1992; 19(10):410-412.
11. R H Dababneh, A Khouri, M Addy. Dentine hypersensitivity-an enigma? A review of terminology, mechanism, aetiology and management. British Dental Journal 1999; 187:606-611.
12. Burwell A, Jennings D, Muscle D, Greenspan DC. Novamin and dentin hypersensitivity- in vitro evidence of efficacy. J Clin Dent 2010; 21(3):66-71.
13. Earl JS, Leary RK, Muller KH, Langford RM, Greenspan DC. Physical and chemical characterization of dentin surface following treatment with novamin technology. J Clin Dent 2011; 22(3): 62-67.
14. Gilliam DG, Tang JY, Mordan NJ, Newman HN. The effects of novel Bioglass dentifrice on dentine sensitivity: a scanning electron microscopy investigation. J Oral Rehab 2002; 29(4):302-313.
15. Forsback AP, Areva S, Salonen Jl. Mineralization of dentin induced by treatment with bioactive glass S53P4 in vitro. Acta Odontol Scand 2004; 62(1):14-20.
16. Di MQ, Bian Z, Jiang H, Greenspan DC, Burwell AK, Zhong J et al. Clinical evaluation of a dentifrice containing calcium sodium phosphosilicate (novamin) for the treatment of dentin hypersensitivity. Am J Dent 2008; 21(4): 210-214.
17. Irene P, Rod H, Mike S, Stacey L, Lynette Z, Diane C. A breakthrough therapy for dentin hypersensitivity: How dental products containing 8% arginine and calcium carbonate work to deliver effective relief of sensitive teeth. J Clin Dent 2009; (sppIss): 23-31.
18. Uraz A, Erol- SImsek O, Pehlivan S, Suludere Z, Bal B. the efficacy of 8% arginine-CaCO3 application on dentine hypersensitivity following periodontal therapy: A clinical and Scanning electron microscopic study. Med Oral Patol Oral Cir Bucal 2013; 18(2):298-305.
19. Koukichi M, Yuichi K. Laser therapy of dentin hypersensitivity. J Oral Laser Application 2007; 7:7-25.
20. Goharkhay K, Wernisch J, Schoop U, Moritz A. Laser treatment of hypersensitive dentin: comparative ESEM investigations. Journal of Oral Laser Applications 2007;7:211–223.
21. Ishikawa K, Suge T, Yoshiyama M, Kawasaki A, Asaoka K, Ebisu S. Occlusion of dentinal tubules with calcium phosphate using acidic calcium phosphate solution followed by neutralization. J Dent Res 1994; 73(6): 1197-1204.
22. Akatsura R, Ishihata H, Noji M, Matsumara K, Kuriyagawa T, Sasaki K. Effects of hydroxyapatite film formed by powder jet deposition on dentin permeability. Eur J Oral Sci 2012; 120(6): 558-562.
23. Salvatore S, Timothy FW, Ian T. Dentin desensitization induced by prophylactic and air-polishing procedures: An in vitro dentin permeability and confocal microscopy study. Journal of Dentistry 2010; 38: 411-422.
24. Saeed A, Kholood AS, Radd ND. Treatment of dentin hypersensitivity with a combination of nano-fluor-hydroxyapatite and Nd:YAG laser. Int Arab J of Dent 2013; 4(2): 84-88.
|