Introduction
Cigarette smoking is a modern day epidemic that poses substantial health problems.The health consequences of cigarette smoking and the other tobacco products are well known.[1] It has been estimated that tobacco use accounts for more than 90% of oral cancers and smokers have a three-fold increase risk of oral cancer. The smoking associated risk of oral cancer is both dose and duration dependent.[2] Smoking has an effect on the various metabolic and biological processes in the body including secretion of hormones.These are mediated chiefly through behavioural and pharma cological actions of nicotine but also occur as a result of increase in the physical effects of stress on the body caused by smoking.[3] Nicotine probably stimulates hypothalamic cholinergic receptors leading to a release of corticotrophin releasing hormone (CRH) which in turn stimulates ACTH secretion from pituitary corticotrophs with a subsequent cortisol release from the adrenal cortex. Alternatively, nicotine induced vasopressin secretion may lead to ACTH release.[4] Cortisol with several functions in the body also has been implicated in the stress response. When exposed to a stress, the body goes through a series of events which leads to an increase in cortisol production. The paraventricular nucleus of the hypothalamus secretes corticotrophin-releasing hormone in response to the stressor. The corticotrophin-releasing hormone then stimulates the anterior pituitary gland to secrete adrenocorticotropic hormone. This adrenocorticotropic hormone enters the bloodstream and acts on the adrenal glands, causing them to produce cortisol.[5] Cortisol is a stress hormone within the hypothalamic pituitary adrenal axis (HPA) axis, which is influenced by smoking and related to chronic diseases like atherosclerosis, heart diseases, high blood pressure and low grade inflammation. The effect of smoking on cortisol secretion is mild to moderate, but this consistent effect everyday over many years may potentially have large consequences on downstream endocrine function.[6]
Cortisol can be measured in urine, plasma and saliva. Secretion of cortisol in saliva is a passive process and a reliable indicator of serum level. Thus the use of saliva sampling is a reliable, non invasive and easy procedure.[7] Hence the aim of this study is to evaluate salivary cortisol level in cigarette smokers and thereby establish the relationship between elevated cortisol levels in response to smoking and its impact on physical and mental health. Evaluation of salivary cortisol level also helps in the early detection and management of depression, anxiety and stress and encourages tobacco cessation in cigarette smokers.
Materials & Methods
A case control study was undertaken on out patients reporting to the department of Oral Medicine and Radiology and the study was approved by the ethical committee of the institution. 70 healthy subjects included in the study were divided into 2 groups. 35 cigarette smokers with a smoking history of at least 6 months aged between 18 to 70 years & 35 non smokers aged between 18 to 70 years.
 | Image 1 – Armamentarium For Collection Of Saliva
 |
 | Image 2 – Saliva Collection Using Spit Technique
|
 | Image 3 – Containers With Collected Saliva Of The Patients
|
 | Image 4 – Cortisol Kit
|
 | Image 5 – Elisa Wells
|
After the patients were selected based on the above inclusion criteria, the subjects were subjected for saliva collection for cortisol estimation. The subjects were asked not to eat, drink, chew gum or brush teeth for at least 30 minutes prior to saliva collection. Saliva was collected in the morning hours to avoid diurnal variations (9:30 to 10.30 A.M). Approximately 2.0 ml of unstimulated whole saliva was collected from each subject in a sterile container by normal spitting method. The samples were stored at -20º C and maintained at that temperature until shortly before assay. Then psychological evaluation was done using depression, anxiety, stress scale (DASS). This scale enclosed a self assessment questionnaire of 42 questions. Each component of depression, anxiety & stress enclosed 14 questions.
 | Image 6 – Elisa Analyser
|
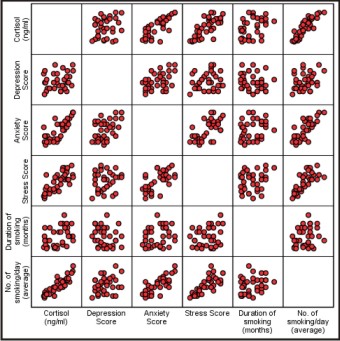 | Scatter Plot – Correlation Between Cortisol & Other Parameters In Group 1
|
Salivary cortisol levels were estimated by Enzyme-linked Immunosorbent Assay (ELISA) method using Cortisol Kit. 1.4 to 10.1 ng/ml of salivary cortisol levels (morning 9.30-10.30 am) is taken as normal range based on this assay. Descriptive and inferential statistical analysis was carried out in the present study. The results on continuous measurements were presented on Mean SD (Standard deviation) (Min-Max) and on categorical measurements were presented in Number (%). Significance was assessed at 5 % level of significance. t -- test was used to find the significance between 2 groups for each parameter. Karl - Pearson correlation (r) was used to assess the relationship between different parameters. A p value of 0.05 or less was considered for statistical significance for the tests. A scatter plot diagram is used to sketch the relation between the variables.Each block shows the data between two variables at a time. The Statistical software namely SPSS 13.0 were used for the analysis of the data and Microsoft word and Excel have been used to generate graphs, tables etc.
Results
According to gender distribution in the study sample Group 1 (smoker) comprises of 31 males & 4 females .Group 2 (non smoker) comprises of 28 males & 7 females. Among males 31(53%) were smokers 28(47%) were non smokers & among females 4(36%) were smokers & 7 (64%) non smokers.The patients included in our study were in the age range of 18 to 70 years. The mean age (years) according to gender and overall in each group was calculated & it was found that in group 1(smokers) among males is 40.84, females 30.00,overall 39.60, in group II ( non smokers) among males 38.04, females 36.14, overall 37.66 years
Salivary cortisol estimation was done in all the 70 patients and the mean salivary cortisol level was calculated. (Table 1 & Graph 1). This shows that higher mean salivary cortisol was recorded in smoker group compared to non smoker group and the difference between them was found to be statistically significant (p < 0.001).
All the 70 patients were subjected to psychological evaluation using DASS scale & the mean depression,anxiety & stress score was recorded.When the mean depression score in smokers and non smokers were compared the difference between them was not statistically significant (P>0.05) .The mean anxiety core was recorded for all the 70 patients based on DASS scale (Table 2) Higher mean anxiety score was recorded in smokers compared to non-smokers and the difference between them was found to be statistically significant (P<0.01). The mean stress score was recorded for all the 70 patients based on DASS scale (Table 3). Higher mean stress score was recorded in smokers compared to non-smokers and the difference between them was found to be statistically significant (P<0.05). Hence it infers from our study that there is a strong association between smoking and stress.
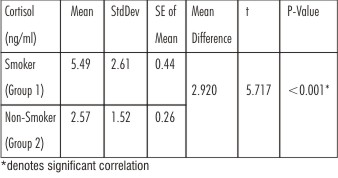 | Table 1: Comparison Of Salivary Cortisol Levels In Group 1 & Group 2 (Ng/Ml)
|
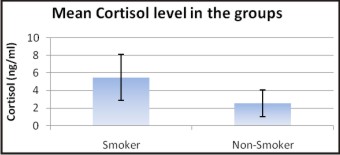 | Graph 1
|
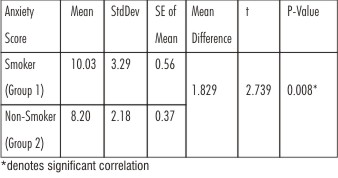 | Table 2: Comparison Of Anxiety Score In Group 1 & Group 2
|
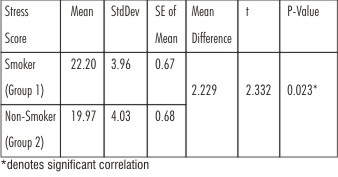 | Table 3: Comparison Of Stress Score In Group 1 & Group 2
|
Karl - Pearson Correlation between cortisol & other parameters in each group was done. In group 1 (Smokers) salivary cortisol level is strongly associated with anxiety, stress, number of cigarettes smoked/day (Average) and there is no strong association of cortisol with depression & duration of smoking. In group 2 salivary cortisol level is strongly associated with stress & also associated with depression & anxiety (Table 4).
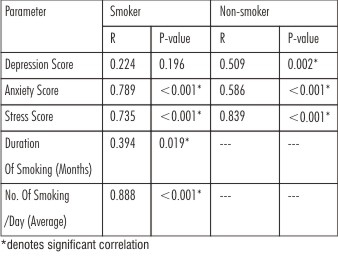 | Table 4: Correlation Between Cortisol & Other Parameters In Group 1 & Group 2
|
Discussion
Smoking is a commonly known risk factor for mental and physical health. Recent reviews of the effects of smoking on endocrine function document that smoking has multiple effects on hormone secretion including effects on the hypothalamic-pituitary-adrenal (HPA) axis. The HPA axis is primarily used in the body’s response to physical and mental stress.[8] A reliable biological marker for HPA axis is increased peripheral cortisol concentration. Cortisol is a stress hormone synthesized by the adrenal cortex which is influenced by smoking and related to chronic diseases.[7]
The relationship between smoking, cortisol and nicotine is important for at least three reasons. First, the HPA axis is implicated in addictive processes. Second, heightened levels of cortisol have a range of adverse effects on biological processes relevant to long-term health.Cortisol may therefore mediate some of the effects of smoking on health, outcomes such as cardiovascular disease and the metabolic syndrome. Third, cortisol is highly sensitive to psychological stress.[9]. Thus a case control study was undertaken on out patients reporting to the department of Oral Medicine and Radiology to evaluate salivary cortisol level in cigarette smokers and thereby establish the relationship between elevated cortisol level in response to stress, anxiety and depression. Since measurement of cortisol is a non invasive & easy procedure, the measurement of cortisol by salivary sampling is advocated in the present study.
It has been hypothesized that stress may also indirectly affect health by increasing the likelihood of health risk behaviours such as smoking. However, evidence on the association between stress and smoking has remained uncertain.[10] Hence the second aim of our study is to show the correlation between salivary cortisol and psychological factors such as stress, anxiety & depression in cigarette smokers. In the current study we used a self reported scale called DASS (depression, anxiety, stress scale). The Depression Anxiety Stress Scale (DASS) is a 42-item self-report measure of anxiety, depression and stress developed by Lovibond and Lovibond (1995) which is increasingly used in diverse settings. Its popularity is partly attributable to the fact that, unlike many other self-report scales, the DASS is in the public domain (i.e. the measure can be used without incurring any charge). This scale enclosed a self assessment questionnaire of 42 questions. Each component of depression, anxiety & stress enclosed 14 questions.
When salivary cortisol level estimation was done among Group 1 & 2 it was found that cortisol level was significantly higher in smokers compared to non-smokers with P<0.001 suggesting a strong significant association.These results support some but not all previous reports of an association between cigarette smoking and increased cortisol secretion.[7],[9],[11] These findings may reflect methodological differences in study design or differences in sample size. A study was done by E Badrick, C Kirschbaum et al in 2007 to establish the relation between smoking status and cortisol secretion. The study concluded that salivary cortisol is increased in current smokers, compared with nonsmokers; no differences were observed between ex smokers and never-smokers, suggesting that smoking has a short term effect on the neuroendocrine system.[7]
On the other hand there are certain studies which do not go in hand with our study results. In an early study of 10 smoking and 15 nonsmoking premenopausal women, Yeh and Barbieri (1989) found no differences in 24-h urinary cortisol excretion levels.[12]
Karl - Pearson Correlation between cortisol with duration of smoking & no of smoking /day (average) was done. In our study we found that salivary cortisol level is strongly associated with no of cigarettes smoked /day (average) but not with duration of smoking. Our study results are in favor of some of the previous studies which also states that there are no long term effects of smoking on cortisol secretion and that the effect of smoking on cortisol changes after quitting[7],[13]. According to the study done by Nese Direk to examine the association between short and long-term indicators of smoking and cortisol levels suggested that the effects of smoking on cortisol are not permanent.[8]
All the 70 patients (Group 1 & 2) were also subjected to psychological evaluation using DASS scale & the mean score was recorded. Higher mean depression score was recorded in smokers compared to non-smokers but the difference between them was not statistically significant (P>0.05), higher mean anxiety score was recorded in smokers compared to non-smokers and the difference between them was found to be statistically significant (P<0.01).Thus our study found a strong co relation between smoking and anxiety. The results also showed that higher mean stress score was recorded in smokers compared to non-smokers and the difference between them was found to be statistically significant (P<0.05) indicating that smoking is associated with increase in stress.
A study done by Sheldon Cohen et al provided evidence of the possible role that stress plays in smoking post withdrawal relapse. It had also added a dynamic aspect to existing work in this field providing the first evidence that changes in smoking status among persons trying to quit are associated with changes in perceived stress level.[14]
Another study was done by Anne Kouvonen et al to examine the relation between work stress, as indicated by the job strain model, and the effort-reward imbalance model, and smoking suggested an association between work stress and smoking and implies that smoking cessation programmes may benefit from taking into account the modification of stressful features of work environment.[10] The result hinted at a positive association between stress, anxiety and overall cortisol levels and suggested that morning cortisol is a sensitive indicator of stress & anxiety. On the contrary several studies have shown no significant relationship between cortisol patterns and stress levels across individuals.[15] There is substantial literature that has identified cortisol level in populations under stress & many investigations have failed to replicate this association. Reasons could be inconsistent methodology, time factors etc.Therefore inherent variability in cortisol levels both between & within individuals could be due to gender differences, effect of time of day, medication, food intake & differences in analytical approach.[16]
Nicotine-induced cortisol secretion may act directly upon central nervous structures in order to change processes like attention, memory, or mood. Such effects have been observed in several studies probably reflecting some of the biochemical changes which may reflect the "gratifications of smoking”. In contrast, adverse effects of chronically elevated cortisol levels may include suppression of parameters of the immune system like natural killer cell activity or a reduced responsiveness of the HPA axis to a variety of stimuli. In view of the hypothesis that glucocorticoids prevent the organism from overshooting defense reactions in stressful situations chronic smoking thus could indirectly threaten homeostasis by blocking the glucocorticoid feedback loop. This intriguing hypothesis should be carefully investigated in future studies.
Our observations of increased cortisol levels in smokers compared to non smokers may also provide a useful indicator for exploring the mechanisms by which nicotine-stress interactions are mediated. Systematic research examining the cortisol effects of both fixed dosing and self-administration of nicotine, and varying the temporal relations between stress and nicotine availability, may help to resolve some of the puzzling inconsistencies that characterize the literature on smoking and anxiety in the context of stress.
Conclusion
The present study involved a small sample size and the results of this study needs to be confirmed in large population based longitudinal studies. Further research can be directed on larger population with daily multiple serial salivary cortisol measurements in smokers, non smokers and ex smokers followed up over longer periods of time. This will help to resolve whether the effect of chronic smoking on salivary cortisol may potentially have large consequences on downstream endocrine function. Moreover the impact of salivary cortisol levels on psychosocial factors like depression, anxiety and stress may help in the early detection and management of depression, anxiety and stress and encourages tobacco cessation in chronic cigarette smokers
References
1. Kapoor D, Jones TH. Smoking and hormones in health and endocrine disorders. Eur J Endocrinol 2005; 152:491–499.
2. Gandini S, Botteri E, Iodice S, et al. Tobacco smoking and cancer: a meta-analysis. Int J Cancer 2008; 122 (1): 155-64.
3. Kremen S. William, O'Brien C. Robert, Panizzon S Matthew et al. Salivary cortisol and prefrontal cortical thickness in middle-aged men: A twin study. NeuroImage 2010; 53: 1093–1102.
4. Kirschbaum S. Wrist, C.J. Strasburg. 'Normal' cigarette smoking increases free cortisol in habitual smokers. Life Sciences 1991 ; 50 : 435-442.
5. Miller G.E, Chen E, Zhou E.S. If it goes up, must it come down? Stress and the hypothalamic-pituitary-adrenocortical axis in humans. Psychological Bulletin 2007; 133: 25-45.
6. Direk Nese, Newson S Rachel, Hofman Albert , Kirschbaum Clemens , Tiemeier Henning. Short and long-term effects of smoking on cortisol in older adults. International Journal of Psychophysiology 2011; 80: 157–160.
7. Ellena Badrick, Clemens Kirschbaum, and Meena Kumari. The Relationship between Smoking Status and Cortisol Secretion. The Journal of Clinical Endocrinology & Metabolism 2007; 92(3):819–824.
8. Direk Nese, Newson S Rachel, Hofman Albert, Kirschbaum Clemens, Tiemeier Henning. Short and long-term effects of smoking on cortisol in older adults. International Journal of Psychophysiology 2011; 80: 157–160.
9. Andrew Steptoe, Michael Ussher. Smoking, cortisol and nicotine. nternational Journal of Psychophysiology 2006 ;59: 228 – 235.
10. Kouvonen Anne , Kivimäki Mika , Virtanen Marianna , Pentti Jaana , Vahtera Jussi . Work stress, smoking status, and smoking intensity: an observational study of 46 190 employees. J Epidemiol Community Health 2005; 59:63-69.
11. Field A.E, Colditz G.A., Willett W.C., Longcope C, McKinlay J.B. The relation of smoking, age, relative weight, and dietary intake to serum adrenal steroids, sex hormones, and sex hormone-binding globulin in middle-aged men. J. Clin. Endocrinol 199 7;9:310– 1316.
12. Yeh J, Barbieri RL .Twenty-four-hour urinary-free cortisol in premenopausal cigarette smokers and nonsmokers. Fertil Steril 1989; 52:1067–1069.
13. Spielman A.Interaction of saliva and taste. J Dent Res 1990; 69(3): 838-843.
14. Cohen Sheldon.Percieved stress,quiting smiking & smoking relapse.Health Psychology 1990 ; 9(4) : 466-478.
15. Kurina M Lianne, Schneider Barbara and Waite J Linda. Stress symptoms of depression and anxiety, and cortisol patterns in working parents. Stress and Health 2004; 20: 53–63.
16. Shah B, Ashok L, Sujatha GP: Evaluation of salivary cortisol and psychological factors in patients with oral lichen planus. Indian J Dent Res 2009; 20(3):288-292.
|