|
|
|
| Chromium Allergy In Orthodontics : A Review |
Satnam Singh 1 , Poonam Bali 2 , Sukhraj Singh Saini 3 , Vinaya S Pai 4
1 Senior Lecturer , Dept. of Orthodontics - Institute Of Dental Sciences And Research Centre, Sehora , Jammu
2 Reader, Dept. Of Prosthodontics - Desh Bhagat Dental College , Muktsar, Punjab
3 Professor, Dept. Of Orthodontics - Himachal Pradesh Dental College , Sundernagar, Distt: Mandi, Himachal Pradesh,
4 Professor And Hod, Dept. Of Orthodontics - Bangalore Institute Of Dental Sciences And Research Centre, Bangalore , Karnataka.
|
| Address For Correspondence |
Address For Correspondence:
Dr. Satnam Singh, Senior Lecturer,
Dept. Of Orthodontics,
Institute Of Dental Sciences, Sehora,
Kunjwani-bishnah Road, Jammu, Jammu And Kashmir.
Mobile No: 08437226555
Emailid : satnamdr555@yahoo.com |
| Abstract |
| The incidence of allergies in general is on the increase. An allergic reaction can also occur during any dental and orthodontic treatment. However, the allergic potential of orthodontic appliances is frequently overestimated. Nickel is the most common metal to cause contact dermatitis in orthodontics. Chromium and Nickel-containing metal alloys, are widely used in orthodontic appliances. An allergic reaction to methylmethacrylate self-curing acrylic resin during orthodontic treatment also had been noticed. A localized hypersensitive reaction appeared on the palate after an orthodontic retainer was placed. In general, the most significant human exposure to nickel, chromium and titanium occures through diet, atmosphere, drinking water, clothing fastners, jewelry and iatrogenic uses of articles containing these metals.Since, the oral environment is particularly ideal for the biodegradation of these metals because of its ionic, thermal, microbiologic and enzymatic properties, some level of patient exposure to the corrosion products of these alloys could be assumed, if not assured. |
|
| Keywords |
| hypersensitivity, dermatitis, leukocyte migration |
|
| Full Text |
Introduction
An increasing concern with the biocompatibility of dental materials , might be due to an increase in the frequency of allergic reactions to materials or to an increase in awareness of adverse effects of these materials. Orthodontic bands , brackets and wires universally made of austenitic stainless steel containiing approximately 18% chromium and 8% nickel. Nickel is the most common cuase of metal induced allergic contact dermatitis in man and second in frequency is chromium.
According to Rahilly. G[1], nickel is the most common metal to cause contact dermatitis in orthodontics. Nickel-titanium alloys may have nickel content in excess of 50 per cent and can thus potentially release enough nickel in the oral environment to elicit manifestations of an allergic reaction.
Another study by Lilian Staerjkaer[2] stated that the nickel is the most common contact allergen affecting females in Europe and the USA. Nickel-containing metal alloys are extensively used for dental prostheses and orthodontic appliances.
The findings of this study did not indicate that nickel sensitive persons are at greater risk of developing discomfort in the oral cavity when wearing an intraoral orthodontic appliance.
The average dietary intake of three metals has been estimated to be 200 to 300 ug/day for nickel ,280ug/day for chromium and 300 to 2000 ug/day for titanium. Nickel concentrations in drinking water generally measures below 20ug/L. 0.43ug/L is reported to be average chromium level in drinking water and for titanium levels are reportrd to range from 0.5 to 15 ug/L.[3]
According to Faribroz.A[4] the mean salivary nickel (Ni) content in subjects with and without a fixed orthodontic appliance was 18.5 ± 13.1 and 11.9 ± 11.4 ng/ml, respectively. The mean salivary chromium (Cr) ion level recorded was 2.6 ± 1.6 ng/ml in the study group and 2.2 ± 1.6 ng/ml in the control group. Within the limits of this in vivo study, it is concluded that the presence of fixed orthodontic appliances leads to an increased concentration of metal ions (Ni and Cr) in salivary secretions.
Ramandan[5] determined the effect of chromium and nickel on gingival tissues during orthodontic treatment and concluded that the patients showed allergic reaction after 3 months of appliance placement and this had disappeared by 1 month after appliance removal. The allergy to either to nickel or chromium is not a serious medical problem, oral hygiene measures in at risk patients should be optimal, with use of flouride free tooth paste and mouth rinse.
To find the incidence of hypersensitivity to orthodontic metals, the patch tests were carried out before and 2 months after the placement of orthodontic appliances in a study by Lucaine MM[6]. Statistically significant positive reactions were observed for nickel sulfate (21.1%), potassium dichromate (21.1%), and manganese chloride (7.9%). Reactions to nickel sulfate had the greatest intensity and even the potassium dichromate. No differences were observed between the reactions before and after placement of orthodontic appliances. The incidence of allergies in general is on the increase. An allergic reaction can also occur during any dental and orthodontic treatment. However, the allergic potential of orthodontic appliances is frequently overestimated.
The incidence of suspected allergic reactions during fixed appliance therapy was determined by questionnaire in which more extraoral (45%) than intraoral (17%) skin changes were registered, with both intraoral and extraoral changes being observed in 38%. Skin changes occurring in the course of orthodontic treatment should be examined and verified if necessary by a dermatologist. Gold plating and other coatings (titanium nitride) of the metal elements even encourage corrosion after a brief protection period. Soldering should be avoided[7].
An allergic reaction to methyl methacrylate self-curing acrylic resin during orthodontic treatment was also noticed. A localized hypersensitive reaction appeared on the palate after an orthodontic retainer was placed. The residual monomer content was between 0.745% and 0.78%, which did not exceed international standards for this material. Patch tests were performed with several methylmethacrylate resin samples showed positive reactions. Despite this many alternative products available, self-curing acrylic resin remains widely used because of its low cost, ease of use, and diversity of indications[8].
According to Sidney AK[9], dietary deficiency of chromium has been associated with-impaired growth and fertility, a diabetic like state connected to impaired glucose tolerance , hyperinsulinemia , hypercholesterolemia , enhanced atherogenesis. Human chromium deficiency has been indisputably proved in protein – calorie malnutrition and in patients receiving total parenteral- nutrition (TPN) devoid of chromium supplements.
Chromium salts were identified as human contact allergens between the two world wars[10].
Toxicodynamic Considerations
Iatrogenic exposures to chromium, nickel and titanium can occur from joint prostheses , dental implants, orthopedic plates and screws, surgical clips and steel sutures , pacemaker leads, prosthetic heart valves, dental alloys and orthodontic appliances.
It has been reported that in vitro release rate for full mouth orthodontic appliances to be 36ug/day for chromium and 40ug/day for nickel. Nickel release from dental alloys have been reported as 4.2 ug/cm2 per day. Heat treated stainless steel orthodontic arch wires showed the release rate for nickel to be 0.26ug/cm2 per day[3].
In a study in which cultured human cells were used, nickel was reported to be moderately cytotoxic while chromium was considerd to have little cytotoxitcity injury to skin from mechanical, physical or chemical agents followed by intimate contact with sensitizing allergens favouring the development of allergic eczematous dermatitis[11].
Diagnosis And Detection Of Chromium Allergy
By following the patients history such as previous allergic response after wearing earring or metal watch strap, appearnce of allergy symptoms shortly after the initial insertion of orthodontic componentc containing nickel and chromium and even confined extraoral rash adjacent to head gear studs, provides allergic response history.
According to Bukhard Summer[12], a study was done to assess the ion release from Cobalt Chromium Molybdenum alloy (CoCrMo) alloy and stainless steel in vitro and the cutaneous reactivity to it by patch test. They concluded that there was low nickel ion release from stainless steel and CoCrMo discs into different elution media. With concomitant eczematous reaction upon patch testing it was found that 5 patients were Cobalt allergic and 3 also of nickel and chromium allergic.
The standard assay for the detection of chromium sensitization , the patch test, does not allow discrimination between patients with and without clinical symptoms of allergy. A study by Lindemann.M[13] aimed to prove whether cellular in vitro tests are predictive of chromium allergy. Chromium sensitized volunteers with and without clinically manifested allergy and non sensitized healthy contorl were analysed by cellular in vitro methods using tri - and hexavalent chromium (chromium chloride and potassium dichromate) as stimuli. Sensitized individuals with an allergy displayed significantly higher lymphocyte transformation test (LTT) responses than volunteers without allergy and controls. Combining the results of chromium chloride and potassium dichromate LTT, a positive reaction to atleast one of stimuli was highly predictive of allergy.
Another study on chromium contact allergy by D.Tio[14] utilized capillary tube leukocyte migration (LMT) inhibition assay as an invitro method for the demonstration of chromium hypersensitivity on clinically proven or suspected chromium allergy individuals. LMT has found wide employement in immunopathology and denote delayed type immunity in man. The results of this study were not influenced by skin allergic reactivity to compounds other than chromium and the method was found to be of practical clinical value for diagnosing chromium allergy.
Biology Of Reaction
Metallic dental appliances consist of dental amalgams (usually in fillings), solid solution chromium alloys (usually in partial plates) and wrought stainless steel wiring (usually in orthodontic or complex bridge work)[15]. Chromium elicits contact dermatitis which is delayed hypersensitive immune response. No symptoms at initial exposure, but subsequent exposure leads to more visible reaction.
Signs And Symptoms
The reaction would be stomatitis from mild to severe erythema , loss of taste, tongue soreness, angular cheilitis, allergic contact dermatitis, widspread eczema and exacerbation of preexsisting eczema. (Fig:1).
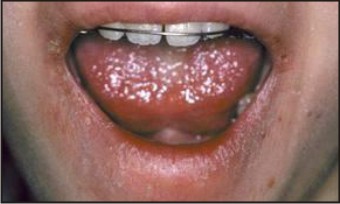 | Figure 1
 |
Many substances used by dental laboratory technicians (occupational toxic risks) can cause either irritation or allergic reactions . Exposure to chromium can cause[16]:
(1) Eczematoid dermatitis with oedema and pruritus particularly in forearm (‘chromium bracelet’)
(2) Mucous cutaneous ulcerations (‘chromium holes’ or ‘tanner’s ulcers’). The most frequent cutaneous localisation is on palm of the hands, while most frequent mucous localisation is the nasal septum due to contamination of hands.
(3) chronic rhinitis, pharyngitis, larygitis and sometimes bronchitis.
(4) asthma in workers exposed to chromic acid fumes and hexavalent chromium derivatives.
Alternatives to prevent chromium allergy in orthodontics would be use of Teflon coated (Tooth coloured epoxy resin) wires, Optifelx archwires, Fibre reinforced composite archwires, Beta III Titanium, CNA Beta - Titanium and TMA wires. These wires too prevent allergic reactions from nickel. Ceramic brackets, polycarbonate brackets, polycrystalline brackets, single crystal sapphire and zirconia brackets ,gold plated brackets and titanium brackets are also helpful to avoid allergic reactions to chromium and nickel both. Plastic coated headgears and glass fibre buccal tubes are also an aid to avoid contact dermatitis[1].
Conclusion
While the sensitivity to any of these elements like chromium, nickel ,titanium, acrylic or any other dental material may not present an extreme medical risk, the orthodontist must be aware of the problem, possess a basic understanding in occurance rate, gender predilection, signs and symptoms of allergic reaction. The orthodontist must be familiar with the best possible alternative treatment modalities to provide the safest, most effective care possible in these cases, maintaining optimal oral hygiene.
References
1. Rahilly G. Nickel allergy and orthodontics. J Orthod 2003; 30(2): 171-174
2. Lilian S. Nickel allergy and orthodontic treatment. Eurp. Journal of orthod. 1990; 12(3): 284-289
3. Robert DB. Biodegradation of orthodontic appliances. Part I. Biodegradation of nickel and chromium in vitro. Am J Orthod Dentofacial Orthop. 1993 ; 103 (1)
4. Fariboz A. Metal ion release from fixed orthodontic appliances-an invivo study. Eurp. Journal of orthod 2011; 181
5. Ramandan. Effect of nickel and chromium on gingival tissues during orthodontic treatment-a longitudinal study.World J orthod 2004;5:230-235
6. Lucaine MM. Hypersensitivity to metals in orthodontics .Am J Orthod Dentofacial Orthop. 2004; 126(1)
7. Schuster. Allergies induced by orthodontic alloys: incidence and impact on orthodontic treatment. Journal of orofacial orthopedics 2004;48-59(12)
8. Tatiana SG. Allergy to autopolymerized acrylic resin in an orthodontic patient. Am J Orthod Dentofacial Orthop 2006; 129(3): 431-435
9. Sidney AK.The Toxicology of chromium with respect to its chemical speciation. 1993; 13(3):217-224.
10. David Basketter . Investigation of threshold for allergic reactivity to chromium. Contact Dermatitis .2001; 44, 70-74
11. Park HY. In vitro release of nickel and chromium from simulated orthodontic appliances. Am J Orthod Dentofacial Orthop. 1983; 84 (2)
12. Burkhard Summer .Patch test reactivity to a cobalt-chromium-molybdenum alloy and stainless steel in metal-allergic patients in correlation to the metal ion release. Contact Dermatitis. 2007;57:35-39.
13. Lindemann M. Detection of chromium allergy by cellular in vitro methods.Clinical and Experimental Allergy. 2008; 38:1468-1475.
14. D.Tio .A study on the clinical application of a direct leukocyte migration test in chromium contact allergy.British Journal of Dermatology. 1976 ;94, 65.
15. Hubler WR. Dermatitis from a chromium dental plate. Contact Dermatitis. 1983;9 377-383.
16. Leon Choel .Occupational Toxic Risks in Denatl Laboratory Technicians. J.Environ.Med. 1999; 307-314.
|
|
|
|
|
|
|