Introduction
The tooth resection procedures are used to preserve as much tooth structure as possible rather than sacrificing the whole tooth[1]. Weine[2] has listed the following indications for tooth resection.
Periodontal indications
1. Severe vertical bone loss involving only one root of multi-rooted teeth.
2. Through and through furcation destruction.
3. Unfavourable proximity of roots of adjacent teeth, preventing adequate hygiene maintenance in proximal areas.
4. Severe root exposure due to dehiscence.
Endodontic and restorative Indications
1. Prosthetic failure of abutments within a splint: If a single or multirooted tooth is periodontally involved within a fixed bridge, instead of removing the entire bridge, if the remaining abutment support is sufficient, the root of the involved tooth is extracted.
2. Endodontic failure: Hemisection is useful in cases in which there is perforation through the floor of the pulp chamber, or pulp canal of one of the roots of an endodontically involved tooth which cannot be instrumented.
3. Vertical fracture of one root: The prognosis of vertical fracture is hopeless. If vertical fracture traverses one root while the other roots are unaffected, the offending root may be amputed.
4. Severe destructive process: This may occur as a result of furcation or subgingival caries, traumatic injury, and large root perforation during endodontic therapy.
a. Strong adjacent teeth available for bridge abutments as alternatives to hemisection.
b. Inoperable canals in root to be retained.
c. Root fusion-making separation impossible.
Hemisection (removal of one root) involves removing significantly compromised root structure and the associated coronal structure through deliberate excision[3]. This procedure represents a form of conservative dentistry, aiming to retain as much of the original tooth structure as possible. The results are predictable, and success rates are high if certain basic considerations are taken into account[4].
Case Report
An eighteen year old girl under going orthodontic treatment was referred to the department for the root canal treatment of the tooth 36. The OPG Xray clearly showed impacted tooth 35 and resorbed mesial root of tooth 36 (Fig 1). After discussion with the orthodontist it was planned to do the root canal treatment of the distal root of tooth 36 and surgical extraction of tooth 35 and hemisection with removal of mesial root of tooth 36.
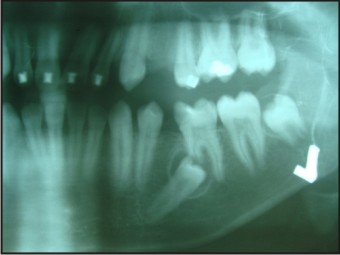 | Fig 1 - OPG Xray showing resorbed mesial root of tooth 36 and impacted tooth 35.
 |
Single sitting root canal treatment was done on the distal root of tooth 36 and and amalgam filling was done (Fig 2).
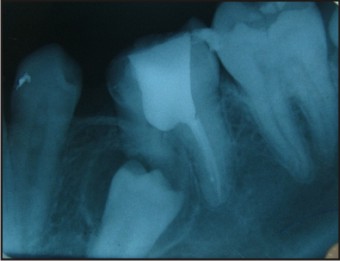 | Fig 2 – IOPA X ray showing obturation of distal root
|
After 1 week tooth 35 was surgically removed and hemisection of tooth 36 was done (Fig 3).
 | Fig 3 – Showing surgical removal of tooth 35 and hemisection of tooth 36.
|
The whole treatment done was later confirmed by an IOPA Xray (Fig 4). A metal ceramic crown was planned later after the completion of orthodontic treatment.
 | Fig 4 – showig IOPA Xray after surgery.
|
Discussion
Hemisection was chosen since patient didn't want a complete extraction. Success of root resection procedures depend, to a large extent, on proper case selection.It is important to consider the following factors before deciding to undertake any of the resection procedures.
Advanced bone loss around one root with acceptable level of bone around the remaining roots.
Angulation and position of the tooth in the arch. A molar that is buccally, lingually, mesially or distally titled, cannot be resected.
Divergence of the roots - teeth with divergent roots are easier to resect. Closely approximated or fused roots are poor candidates.
Length and curvature of roots - long and straight roots are more favourable for resection than short, conical roots.
Feasibility of endodontics and restorative dentistry in the root/roots to be retained.
Various resection procedures described are:
a) Root amputation
b) Hemisection
c) Radisection
d) Bisection
Newell[5] examined 70 root resected molars in 62 patients for the quality of the resections. Twenty-one (30%) of the resections were considered faulty when subgingival, residual roots, furcal lips, and/or ledges were present. Failures were more frequent in maxillary molars (33.3%) than mandibular molars (22.7%). Park et al.[6] have suggested molars that are having questionable prognosis can maintain the teeth without detectable bone loss for a long-term period by hemisection but patient should maintain a good oral hygiene. A study done by Atul Jain[7] on a case of excessive destruction of the mesial root due to the external root resorption and fair amount of the distal root remaining with adequate bone support, hemisection carried out with the removal of the mesial root and crown. Remaining tooth structure was restored with composite and used as an abutment in crown and bridge after repositioning the occlusal contacts in favourable position. Root amputation and hemisection should be considered as another weapon in the arsenal of the dental surgeon, determined to retain and not remove the natural teeth. With recent refinements in endodontics, periodontics and restorative dentistry, hemisection has received acceptance as a conservative and dependable dental treatment and teeth so treated have endured the demands of function[8]. Some investigators[9],[10] reported that root-resected molars had more than 90% survival rate, whereas other investigators[11],[12],[13],[14] reported that ~30% of resected molars failed over a 10-year period. The present case shows an uncommon etiology of resorption of the mesial root of madibular first molar.
Conclusion
Hemisection as a treatment option to conserve the tooth structure and use it as an abutment is still very relevant. The prognosis of root resected molars may not be as grim as previously believed. The results of hemisection are predictable, and success rates are high if certain basic considerations are taken into account. Regular periodontal maintenance and sufficient coronal restoration of the root resected teeth are important precondition for long term survival. Hemisection is an important treatment in the field of dentistry which will help in increasing desire to retain natural teeth.
References
1. Basaraba N. Root Amputation and tooth hemisection.Dent Clin of N Amer 1969;13 : 121
2. Weine FS (1996) Endodontic Therapy. (5thedn).
3. Bühler H (1994) Survival rates of hemisected teeth: an attempt to compare them with survival rates of alloplastic implants. Int J Periodontics Restorative Dent 14: 536-543.
4. Kurtzman GM, Silverstein LH, Shatz PC (2006) Hemisection as an alternative treatment for vertically fractured mandibular molars. Compend Contin Educ Dent 27: 126-129
5. Newell DH. The role of the prosthodontist in restoring root resected molars: a study of 70 molar root resections. J Prosthet Dent 1991;65(1):7-15.
6. Park J. Hemisection of teeth with questionable prognosis. Report of a case with seven-year results. Journal of the International Academy of Periodontology. 2009;11(3):214-9.
7. Jain A, Bahuguna R, Agarwal V. Hemisection as an Alternative Treatment for Resorbed Multirooted Tooth-A Case Report. Asian Journal of Oral Health & Allied Sciences. 2011;1(1):44 6.
8. Haueisen H, Heidemann D. Hemisection for treatment of an advanced endodontic-periodontal lesion: a case report. Int Endod J, 35, 557-572, 2002.
9. Carnevale G, Di Febo G, Tonelli MP, Marin C, Fuzzi M. A retrospective analysis of the periodontal-prosthetic treatment of molars with interradicular lesions. Int J Periodontics Restorative Dent 1991:11:189-205.
10. Carnevale G, Pontoriero R, di Febo G. Long-term effects of root-resective therapy in furcation-involved molars. A 10-year longitudinal study. J Clin Periodontol 1998;25:209-214.
11. Langer B, Stein SD, Wagenberg B. An evaluation of root resections. A ten-year study. J Periodontol 1981; 52:719-722.
12. Buhler H. Evaluation of root-resected teeth. Results after 10 years. J Periodontol 1988;59:805-810.
13. Green EN. Hemisection and root amputation. J Am Dent Assoc 1986;112:511-518.
14. Blomlof L, Jansson L, Appelgren R, Ehnevid H, Lindskog S. Prognosis and mortality of root-resected molars. Int J Periodontics Restorative Dent 1997; 17: 190-201.
|