Introduction
Orthodontic therapy is the most conservative treatment option for malaligned anterior teeth. However, it may be rejected by the patient due to various reasons which include treatment time, financial constraints and appearance during the therapy and relapse after the treatment. Alternatively, endodontic approach combined with the prosthodontics provides a quick, reliable and economic treatment option with no chances of relapse.[1],[2] This case report describes the aesthetic rehabilitation of maxillary anterior teeth in no time using the combined endo prostho approach.
Case Report
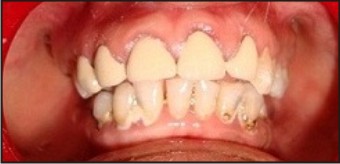
A 40 years old female reported to Department of Oral Diagnosis, J.C.D Dental College, with a chief complaint of severe labial proclination of her maxillary incisors and right canine teeth. She had a convex profile with a lip trap (Fig 1 and 2).
 | Fig. 1 : Showing Severe Proclination Of Anterior Teeth
 |
 | Fig. 2 : Showing Convexity Of Profile
|
She was working as a clerk in a private company. Her periodontal health was good with a non significant medical history. During the treatment planning session, she rejected the orthodontic treatment since she wanted an immediate treatment. The patient was then referred to the departments of prosthodontics and endodontics for aesthetic rehabilitation, where the endodontic treatment of proclined teeth was planned followed by post and core along with full crown coverage. An informed consent of the patient was obtained before commencement of the procedure for the treatment as well as for the publication of this report including images. Preoperative occlusion was analyzed clinically as well as on articulated models (Fig 3). Single visit endodontic treatment of teeth number 6, 7, 8, 9 and 10 was completed under rubber dam isolation (Fig 4). Patient was instructed to take analgesics in case of any pain and was recalled after 5 days to check any postoperative discomfort.
 | Fig. 3 : Showing Diagnostic Models
|
 | Fig. 4 : Iopa Xray Showing Completed Root Canal Treatment
|
In the second appointment, glass fibre posts (Nordin SA Swiss) were placed in the endodontically treated teeth. Patient was asymptomatic during the interappointment period.
During abutment preparation, gross labial reduction was performed to allow the crowns to be fabricated in proper alignment. To reinforce the teeth, composite core build up (Multicore, Ivoclar) was done on the palatal aspect of teeth. The abutment teeth were prepared using the shoulder and chamfer diamond burs (shofu) and crown preparation guidelines (Fig 5).
 | Fig. 5 : Showing Crown Preparation
|
Once the preparation was completed, impressions were taken with polyvinylsiloxane impression material (Aquasil, Dentsply). Impression of the mandibular arch was made with an irreversible hydrocolloid (Jeltrate, Dentsply) and immediately poured with type IV dental stone. Vitapan 3D Master (Germany) shade guide was used for shade determination. Bite registration record was taken, and then the impression was sent to dental laboratory with a written detailed laboratory prescriptionInterim restorations were fabricated with a bis acryl material ( Integrity, Dentsply)and cemented with a temporary luting non eugenol cement. (Freegenol, GC Fuji)
In the next appointment, temporary crowns were removed and all the abutment teeth were cleaned off temporary cement. The metal ceramic crowns were tried in together to assess the marginal fit and contacts. Approval of the patient regarding the shade and shape of the crowns was obtained. Then the crowns were cemented with glass ionomer luting cement (GC Corporation, Japan). Excess luting cement was removed and the marginal area was finished and polished. The final result showed better teeth alignment compared to the initial condition prior to esthetic treatment hence changing the appearance and finally increase patient’s self esteem (Fig 6).
 | Fig. 6 : After Final Cementation
|
The Patient was happy with her new smile and esthetically pleasing view of anterior teeth. She was instructed to maintain a meticulous oral hygiene and a recall appointment was scheduled every 6 months for periodic checkup. No complication was observed during last 2 years of clinical service and patient was satisfied with the results.
Discussion
Pain and aesthetics are the main reasons that bring patient to a dentist. The increasing demand for esthetics has encouraged the practitioners to develop new methods and techniques.[3] Considering esthetic, the best material of choice for matching the natural state of a complex human dentition as in indirect anterior restoration is ceramic for the highly desirable properties in color stability, translucency, light transmission, and biocompatibility.[4],[5],[6]
Nevertheless, patient factors cannot be ignored while treatment planning. Many times adult patients may reject the orthodontic treatment due to the time limitations and socioeconomic factors.[7],[8] As in the present case, patient was not convinced with the orthodontic therapy which was rather most conservative. The only alternative left in this case was then to do endodontic treatment followed by crowns. Endodontic treatment was done on maxillary anterior teeth under consideration of extreme mal-alignment, therefore crowns and posts as intra canal retentions were needed to correct the position of those anterior dentition, with regard that endodontic treatment has high success rate.[9],[10]
As the case involved anterior teeth, patient was explained about the all ceramic crowns for better esthetics.[11] However, for financial reasons, she preferred metal ceramic crowns.
Since there are many different philosophies and technologies that can be applied to esthetic rehabilitation cases, dentists must enrich themselves with thorough understanding about recent technologies and materials, and with that would come a greater ease in providing esthetic services with satisfactory results for the patients.[12]
Conclusion
The art and science of dentistry is devoted to restore and enhance the natural beauty of smile. With adequate multidisciplinary teamwork, it is possible to reestablish a pleasing, healthy functioning smile which will boost the patient confidence. However, patient’sgeneral conditions and expectations should always be considered during treatment planning.
References
1. Kim J, Chu S, Gürel G, Cisneros G: Restorative space management: treatment planning and clinical considerations for insufficient space. Pract Proced Aesthet Dent 2005, 17:19-25.
2. Toh CG, Setcos JC, Weinstein AR: Indirect dental laminate veneers- an overview. J Dent 1987, 15:117-124.
3. Sadowski SJ: An overview of treatment considerations for esthetic restorations: A review of the literature. J Prosthet Dent 2006, 96:433-442.
4. Powers JM, Sakaguchi RL. Craig’s restorative dental materials. 12thed. Philadelphia: Elsevier Inc; 2006. p. 454–6.
5. Roulet JF. Indirect aesthetic restorations. Journal of Advances in Aesthetic and Restorative Dentistry 2003; 5:15–9.
6. Shillingburg HT, Hobo S, Whitsett LD, Jacobi R, Brackett SE. Fundamentals of fixed prosthodontics. 3rd ed. Chicago: Quintessence publishing 2006. P 433-66
7. Suha T, Kivanc U. Esthetic rehabilitation of crowded maxillary anterior teeth utilizing cearmic veneers: a case report. Case journal 2009, 2:8329
8. Javaheri D: Considerations for planning esthetic treatment Assoc with veneers involving no or minimal preparation. J Am Dent 2007, 138:331-337
9. Summitt JB, Robbins JM, Hilton TJ, Schwartz RS. Fundamentals of operative dentistry: a contemporary approach. 3rd ed. Chicago: Quintessence Publishing; 2006. p. 571–84.
10. Shabahang S. State of the art and science of endodontics. J Am Dent Assoc 2005; 136(1): 41–52
11. Prasetyo EP. Esthetic management for anterior teeth: a case report. Jakarta: APDC Publishing; 2007. p. 123
12. lunardhi G.J, Prasetyo E P. Esthetic rehabilitation of crowded and protruded anterior dentition Vol. 42. No. 1 January–March 2009
|