Introduction:
Bell’s palsy affects the unilateral facial muscles with typical features like inability to blink, absence of wrinkles on the forehead and asymmetry of face. The problems encountered during prosthodontic rehabilitation include uncontrolled flow of saliva, a mask-like expressionless appearance and cheek biting. All features may interfere with steps in impression making, jaw relation and denture retention and stability.[1] Palliative treatment for permanent facial paralysis includes, modifications of denture to provide support to cheek like padding for buccal flanges, spring loaded acrylic flanges and magnet retained cheek plumpers.[2] The neutral zone technique is also an alternative to these complex cases. The positioning of artificial teeth in neutral zone achieves two objectives. First, the teeth will not interfere with the normal muscle function, and second, the forces exerted by the musculature are more favourable for stability and retention.
Case Report:
A 58-years-old completely edentulous female patient was presented with facial paralysis of left half of the face with the duration of illness for more than 10 years. Her chief complaints were inability to chew and unaesthetic appearance of face. She was wearing upper and lower complete dentures since 6 years. She had an asymmetric face with loss of muscle bulk (droop) on the paralyzed side (Fig 1). The face was drawn to the right side during phonation. She was not able to close her left eye completely. The primary impressions were made with impression compound and casts were obtained. Border molding was done on special trays and final impressions were made with addition silicon impression material. Extra wax was added on the denture base on the paralyzed side of the face to have facial symmetry and to provide support for the musculature labially and bucally. The jaw relations were recorded and casts were mounted at the established vertical dimension of occlusion. The wax was removed from the lower occlusal rim leaving behind four occlusal stops, two posterior and two in anterior region to maintain the vertical dimension (Fig 2). Neutral zone was recorded with viscogel tissue conditioner material as it is mucostatic and does not apply pressure on soft tissue like impression compound.[3] It can be further added afterwards if first application is not enough to mold material in neutral zone. Its long setting time gives enough time to perform all the functional movements during muscle-molding procedure. Thick mix of viscogel tissue conditioning material was loaded on the lower denture base and patient was asked to smile, grin, pout/purse lips, count from 60 to 70, talk aloud, pronounce the vowels, sip water, swallow, slightly protrude the tongue and lick the lips. These actions were repeated for 10 minutes until material set. The neutral zone thus recorded was more labially and buccaly placed on the paralysed side (Fig 3). The denture base was placed on master cast and silicon putty index was made around the neutral zone (Fig 4). The viscogel material was then removed from denture base and wax was poured in the index that gave the exact representation of neutral zone (Fig 5). Teeth arrangement was done with the help of index and the denture was fabricated in a conventional manner (Fig 6 & 7).
 | Fig 1 : Pre Treatment
 |
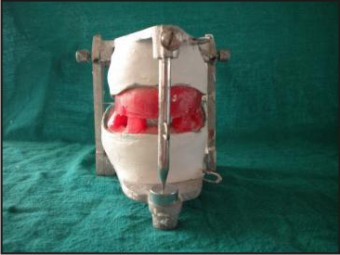 | Fig 2 : Four Occlusal Stops For Maintaining Vertical Dimension
|
 | Fig 3 : Neutral Zone Recorded With Tissue Conditioner
|
 | Fig 4 : Silicone Putty Index
|
 | Fig 5 : Wax Poured In The Index
|
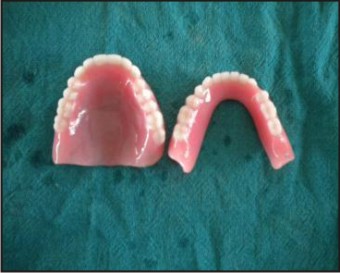 | Fig 6 : Finished Denture
|
 | Fig 7 : Post Treatment
|
Discussion:
Facial palsy is indicative of neurological involvement. Patients with this disease can be treated but it is essential that they understand their problems. Denture retention, maxilla-mandibular relation records and supporting the musculature are some of the added denture problems.[4] The neutral-zone philosophy is based upon the concept that for each individual patient there exists within the denture space a specific area where the function of the musculature will not unseat the denture and where forces generated by the tongue are neutralized by the forces generated by the lips and cheeks. The influence of tooth position and flange contour on denture stability is equal to or greater than that of any other factor. We should not be dogmatic and insist that teeth be placed over the crest of the ridge, buccal or lingual to the ridge. Teeth should be placed as dictated by the musculature, and this will vary for different patients. Flaccid facial muscles needed support and this was done by adding wax. The additional material could be easily added since muscular force exerted against it by the paralyzed muscle and tissues were no longer a deterrent factor. The dentures should provide the patient with improved facial appearance, stability and retention during function as they have been constructed in harmony with their surroundings.[5] The technique is relatively simple but there are increased chair time and laboratory cost.[6] It was important that the remaining oral structures be maintained in a state of good health so that the prosthesis lasts longer. Since the food accumulates on the paralyzed side, the patient was instructed to maintain the hygiene of the prosthesis and oral cavity. Regular gum massage was advised to maintain the supporting tissues in a state of good health.[7]
Conclusion:
The neutral zone concept is an alternative technique for the construction of lower complete dentures in case of facial paralysis patients. These modifications improved esthetics and function with complete dentures.
References
1. Hussain S, Jayesh R, Nayar S, Aruna U, Abraham AM. Prosthodontic management of a completely edentulous patient with Bell’s palsy. Indian Journal of multidisciplinary dentistry 2011; 2(1):404-6.
2. Fickling BW. Buccal sulcus supports for facial paralysis. Br Dent J 1951;90 (5):115-7.
3. Kursoglu P, Ari N, Calikkocaoglu S. Using tissue conditioner material in neutral zone technique. NYSDJ 2007; Jan: 40-42
4. Heartwell CM, Rahn AO. Syllabus of complete dentures: Diagnosis 4th Ed; Varghese Publishing House, 1984: 109-110.
5. Beresin V, Schiesser FJ. The neutral zone in complete dentures. J Prosthet Dent 2006; 95: 93-101.
6. Gahan MJ, Walmsley AD. The neutral zone impression revisited. Br Dent J 2005; 198: 269-72.
7. Pandey S and Datta K. Prosthodontic management of a completely edentulous patient with unilateral facial paralysis. Journal of Indian Prosthodontic society 2007; 7: 211-213.
|