Introduction
Early childhood caries is a life style disease that begins as soon as the child’s first teeth erupt into the oral cavity. The process is attributed to poor oral hygiene, on demand feeding and developmental defects that increase t he susceptibility of teeth to caries[1]. Depending on the chronology of eruption the process involves the deciduous anterior teeth first followed by the molars. The extent of decay of teeth in Nursing Bottle Caries is usually so severe, that by the time the child is brought to the dentist, much of the anterior clinical crowns are decayed or lost. Decay is associated wit h pain and abscess formation that may further cause bone loss, periodontal involvement mobility. The nutrition and general health of the child is also affected greatly
Treatment options for restorable teeth include cleaning and obturation of root canals followed by crown buildups that involves a variety of procedures like short composite posts, fiber reinforced composites, omega loops and biological restorations. However all these procedures demand cooperation of the young child and increased chair side time. Besides it is seen that the frequency of relapse is more in these teeth leading to sinus formation and abscess. Also the clinical longevity of these restorations is questionable depending on tooth structure available, operator skills and isolation methods used.
Often the decay and subsequent periapical involvement is so severe that the condition demands extraction of the anterior root stumps at an early age. Literature review suggests that missing anterior teeth lead to a number of problems. According to Graber arch length reduces after the premature loss of primary incisors. This is true especially if they are lost early before the eruption of primary canines or if the primary dentition is a closed dentition or t here is deep overbite of incisors. Thus early loss of anterior teeth demands space maintenance[2]. Studies show that significantly large proportion of children with missing or abnormal upper incisors misarticulate sounds compared to the dentate population[3]. Besides early loss leads to development of deleterious oral habits like tongue thrusting leading to malocclusion in the permanent dentition. Children who attend day care may become more aware of their image and lack of teeth. It leads to low self esteem due to compromised esthetics.
Contrary to the assum ption that early extractions may interfere with mastication, studies show that many children indeed show an improved ability to eat and f unction, because t he badly decayed or inf ected teeth inflict pain on eating[4].
Unlike adults where adjacent teeth can be used as abutment for fixed bridges, a similar design hinders the increase in intercanine width during the growth and development of child. Implants are also contraindicated as they interfere with developing tooth bud. Besides since the prosthesis is tem porary and lasts only till the eruption of the ant erior teeth, t he cost of the treatm ent involved becomes an important consideration for treatment.
Hence this paper reviews few appliances that offer more economic alternative for temporary replacement of the missing anterior teeth till the perm anents erupt, require minimum chair side time and child cooperation.
Soldered wire in tube appliance : It is a modificat ion of soldered pin and tube appliance as given by Finn [5].Instead of prefabricated pre-fitted pin and tube appliance a conventionally adapted wire is used in conjunction with a molar tube.
Fabrication : Stainless steel bands are adapted to the abutment teeth. Wire is adapted onto the lingual surfaces, one end of which is soldered and other end is made to passively fit into the molar tube. Onto the wire an acrylic tooth can be bonded depending on the esthetic demands of the patient. (Fig 1,2).
 | Fig 1 : Soldered Wire In Tube Appliance (Labial View)
 |
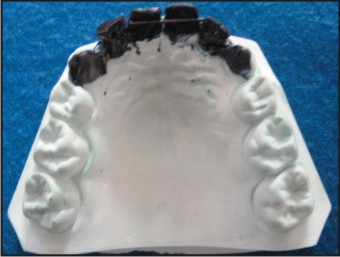
 | Fig 2 : Soldered Wire In Tube Appliance (Palatal View)
|
Advantages : The wire is allowed to slide partially out of the tube in response to lateral growth. A removable passive acrylic tooth can be bonded fulfilling esthetic requirements. Appliance allows adjustment of teeth and stimulation of gingiva over the un-erupted tooth hastens eruption.
Disadvantages
Bands on abutment teeth may interfere with esthetics.
Fixed acrylic partial denture
The design and fabrication is adapted from Brauer’s technique of fixed ceramic denture fabrication[6]. Instead of ceramic tooth colored acrylic can be used. Considering the short time span of service that is required, decreased masticatory loads compared to the permanent dentition, the method offers a more economic alternative.
Fabrication : Abutment teeth are prepared to receive either a full coverage crown or lingual wings. Wax pattern is made f or the fixed partial dent ure and split in the midline. A thin pencil lead coated with Vaseline is passed through the teeth.(Fig 3) Pattern is invested, wax burned out and replica poured with tooth colored acrylic. (Fig 4i, 4ii, 4iii) The lead stick is replaced with 20 gauge wire. The teeth are separated in the midline that accommodates for growth and increase in inter-canine width.
 | Fig 3 : Wax Pattern for Fixed acrylic partial denture
|
 | Fig 4i : Missing 52,51,61,62
|
 | Fig 4ii : Fixed acrylic partial denture (Labial View)
|
 | Fig 4iii : Fixed acrylic partial denture (Palatal View)
|
Advantages : Allows for increase in inter-canine width Fixed alternative that does not interfere with oral hygiene practices
Disadvantages : Requires preparation of the abutment tooth Nance Palatal arch with anterior extension-It is a modificat ion of Nance palatal arch [7]. It acts a as a space maintainer and simultaneously. It acts a as a space maintainer and simultaneously Fabrication- Bands are adapted on 2nd deciduous molars for anchorage. A palatal arch is made using 19 gauge wire. A U shaped loop is incorporated in the arch. The acrylic Nance button has an anterior extension that incorporates artificial teeth. (Fig 5i, 5ii, 5iii).
 | Fig 5i : Missing 52,51,61,62
|
 | Fig 5ii : Nance Palatal arch with anterior extension
|
 | Fig 5iii : Intraorally inserted Nance Palatal arch with anterior extension
|
Advantages : Does not interfere with increase in inter-canine width Maintains space along with offering esthetic replacement
Disadvantages : Interf eres with oral hygiene maintenance Extended Pal atal arch. A modification of Gropers appliance[8]. It provides the good esthetic results, maintains space and allows cleaning thus favoring oral health in general and mucosal health in particular.
Fabrication : A 19 gauge wire arch is adapted along the ridge in upper anterior region which is soldered to bands adapted on 2 deciduous molars. Orthodontics brackets are soldered to wire and acrylic teeth attached to the meshed surface of the brackets. (Fig 6,7).
 | Fig 6 : Extended Palatal Arch (Labial View)
|
 | Fig 7 : Extended Palatal Arch (Palatal View)
|
Advantages : Since deciduous dentition shows over jet of 2mm usually and minimal overbite palatal arch does not interfere with occlusion. It offers a design that allows good cleaning thus facilitating oral hygiene.
Disadvantages : At times the solder joint between the bracket and wire fails leading to loss of artificial tooth attached to the respective bracket.
Removable Partial Denture : It gains its anchorage from both the teeth and the palate. The various modifications range from acrylic dentures, acrylic with wrought wire clasps, and acrylic with cast metal clasps and acrylic saddle with cast metal framework.
Fabrication : Adams / Clasps are used for anchorage from the posterior teeth. Missing teeth are initially stabilized in base plate waxed on the working model. The assembly is then invested and wax replaced with heat cure acrylic.
Advantages : Easy to maintain oral hygiene Minimal chair side time Stimulates gum tissues facilitating early eruption of successors
Disadvantages : Wear depends on patient compliance. Do not emot ionally appeal to the children.
Discussion
Removable or fixed prosthesis can be used t o replace deciduous anterior teeth in children that have been prem aturely lost due to disease. The main consideration while planning these appliances is the dental age of the child. Studies show that if the teeth are lost very early i.e. before t he eruption of deciduous canines, it can lead to space loss in the anterior region; thus necessitating the use of space maintainer [2]. However if the teeth are lost after 3 years of age the decision to place these appliances has to be based upon parental desire, acceptance by the child and the approximate time for the permanent successors to erupt.
Disto-labial migration of canines is an important event in the development of occlusion that allows for alignment of permanent incisors. Thus it is important that the design of these appliances allows increase in the inter-canine width. Unlike permanent t eeth deciduous canine can not be used as abutment teeth. Therefore appliances incorporate deciduous molar banding that permits free migration of canines or when the anteriors are banded sliding mechanisms are incorporated in the design that allow increase in the inter-canine arch width.
The clinical sit uations which contraindicate placement of these appliances are seizure disorders and mental retardation, as these children demonstrate increased occlusal stresses t hat may compromise the longevity of the appliances. In these situations loss, breakage or failure may pose a risk of aspiration. Besides special care should be taken regarding cleaning of these appliances while placing in immune-compromised patients. Some patients report of allergy to acrylic monomer which also precludes the use of these appliances. Also occlusal discrepancies like deep overbite, increase overjet or reverse overbite limit their use.
Once placed in the oral cavity maintenance of adequate oral hygiene is very important. This calls f or regular reinforcement of oral health behavior in children. The first recall visit should be scheduled after 7 days appliances placement. It is usually seen that at this time patients show increased plaque deposition as they get accustomed t o the cleaning of the appliance. Besides evaluating the oral cavity for signs of appliance impingement , oral hygiene instructions should be reinforced. Next the patient can be recalled after a month to check for the integrity of the appliance. Thereafter the patient is regularly examined every six months till the eruption of permanent teeth.
The appliance can be left in the oral cavity till the eruption of the succedaneous teeth. Usually patients report of gingival irritation and pain when teeth pierce the oral mucosa. Other wise the appliance can be removed corresponding to the normal exfoliation time of teeth. Children comfortably fit into the clinical situation as the peers also are in the process of eruption and shedding of teeth.
Clinical experience shows that the appliance usually does not pose much breakage problems except for occasional failure at the solder joint of band and wire. Rarely does the acrylic get abraded or discolored when the appliance is left in the oral cavity for a very long time. Decalcification of the banded tooth and mucosal inflammat ion are other associated problems.
Conclusion
Besides enhancing the facial esthetics anterior prosthesis also act as functional space maintainers, assist in developm ent of proper speech; prevent development of any untoward oral habits thus aiding sound development for the child during the foundation years.
References
1. Quinonez RB, Keels MA, Vann WF, McIver FT, Heller K. Early childhood caries: Analysis of Psychosocial and Biological factors in a high risk population. Caries Research 2001; 35:376-383.
2. Moyers RE, Riolo ML. Handbook of orthodontics. 4 ed. Yearbook medical publishers.Inc., Chicago, London and Boca-rat on: 361.
3. Snow K: Articulation proficiency in relation to certain dental abnormalities. J. Speech Hearing Dis 1961; 26:209-212.
4. Koroluk LD, Riekman GA. Parental perceptions of the effects of maxillary incisor ext ractions in children with nursing caries. ASDC J Dent Child 1991; 58(3):233-236.
5. Finn SB, Hitchcock HP. 2003 Clinical Pedodontics. 4 ed. WB Saunders USA: 352-353.
6. Brauer JC. Dentistry f or children.5 ed. Newyork, Mc Graw-Hill Book Co., Inc., Blakiston Division: 352-353.
7. Dean JA, Mc Donald RE, Avery DR. Dentistry for child and adolescent. 8 ed. Mosby, St. Louis, Missoure: 641.
8. Jasmine JR, Groper JN. Fabrication of a more durable fixed anterior est hetic appliance. ASCD J Dent Child 1984; 51(2):124-127.
9. Dean JA, Mc Donald RE, Avery DR. Dentistry for child and adolescent. 8 ed. Mosby, St. Louis, Missoure: 638.
|