|
|
|
| Taurodontisim In Permanent Molars : A Case Report |
Sanjeev Srivastava 1 , H.S. Chhabra 2 , Kshiti Bhardwaj 3 , Rohit Grover 4
1 Head Of Department, Department Of Conservative Dentistry And Endodontics - Sardar Patel Post Graduate Institute Of Dental And Medical Sciences
2 Reader , Department Of Conservative Dentistry And Endodontics - Sardar Patel Post Graduate Institute Of Dental And Medical Sciences
3 Lecturer , Department Of Conservative Dentistry And Endodontics - Sardar Patel Post Graduate Institute Of Dental And Medical Sciences
4 Reader , Department Of Conservative Dentistry And Endodontics - Sardar Patel Post Graduate Institute Of Dental And Medical Sciences
|
| Address For Correspondence |
Dr. Sanjeev Srivastava
Flat No 310, Ashoka Apartment,
5 Way Lane, Lucknow 226001
Emailid : sanjeevsrivastava409@gmail.com
Mobileno : 9415064214 |
| Abstract |
| Taurodontism can be defined as a change in tooth shape caused by the failure of Hertwig’s epithelial sheath diaphragm to invaginate at the proper horizontal level. An enlarged pulp chamber, apical displacement of the pulpal floor, and no constriction at the level of the cement enamel junction are the characteristic features. Although permanent molar teeth are most commonly affected, this change can also be seen in both the permanent and deciduous dentition, unilaterally or bilaterally, and in any combination of teeth or quadrants. Presented in this case report is a case of bilateral taurodontism in permanent molars. |
|
| Keywords |
| Endodontic treatment, Enlarged pulp chamber, Syndrome, Taurodontism. |
|
| Full Text |
Introduction
The term taurodontism was first introduced by Sir Arthur Keith in 1913[1].The term taurodontism comes from the Latin term tauros, which means ‘bull’ and the Greek term odus, which means ‘tooth’ or ‘bull tooth’[1]. It refers to a tooth form characterized by an external block configuration with an elongated body tending to enlarge at the expense of the root.The taurodontic teeth are identified by elongated pulp chambers and apical displacement of bifurcation or trifurcation of the roots. Due to this, the chamber has a greater apicoocclusal height and lacks the constriction at the level of the CEJ giving it a rectangular shape. So the distance from the bifurcation of roots to the CEJ is greater than the occluso cervical distance[2]. Etiology of taurodontism is failure of Hertwig’s epithelial sheath diaphragm to invaginate at the proper horizontal level. Autosomal transmission of the trait has also been observed[3],[4] Taurodontism can occur alone limited to one or more teeth or it can be associated with various syndromes like Down’s syndrome, Klinefelter’s syndrome etc[5].Taurodontism may be unilateral or bilateral and affects permanent teeth more frequently than primary teeth. It is commonly observed among the Eskimos and Natives of Australia and Central America.Taurodontism can be classified as mild, moderate and severe (Hypo, Meso and Hyper respectively) based on the degree of apical displacement of the pulpal floor.[6],[7]
Despite the clinical challenges in endodontic therapy, taurodontism has received a little attention from clinicians. In performing root canal treatment on such teeth, one should appreciate the complexity of the root canal system, canal obliteration and configuration, and the potential for additional root canal systems. Careful exploration of the grooves between all orifices particularly with magnification, use of ultrasonic irrigation; and a modified filling technique are of particular use. Presented in this article is a case of bilateral taurodontism.
Case Report
A 17 year old male patient reported to the dental clinic with the chief complaint of pain in lower left posterior and upper right region since one month.Patient’s medical history was non contributory.Clinical examination showed normal soft tissue appearance. Lower and upperfirst molar had large carious lesion with pulpal involvement.Orthopantamograph revealed that both molars were with enlarged pulp chambers and short roots suggesting taurodontism (Fig.1.1). No other obvious anomalies were noticed on the Orthopantamograph.Intra oral Periapical radiograph of both sides showed enlarged pulp chamber with short roots (Fig 1.2, 2.0). Based on the clinical and radiographic findings, a diagnosis of chronic pulpitis was made in relation to maxillary right first molar and mandibular left first molar.
 | Fig 1.1 – Pre Operative Opg
 |
 | Fig 1.2 – Pre Operative Iopa Radiograph – 36
|
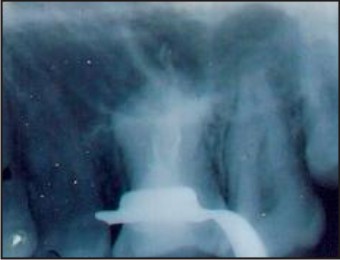
 | Fig 2.0 – Pre Operative Iopa Radiograph – 16
|
Endodontic Management
The tooth was anaesthetized, the access was opened under rubber dam .Pulp tissue was extirpated. The pulp was voluminous and to ensure complete removal, 3% of sodium hypochlorite wasused as an irrigant to soften thepulp. Once the pulp was extirpated, further irrigation was done with normal saline. The pulp chamber was huge and the floor of the chamber could not be visualized,which on further exploration in the apical furcation area revealed two divisions one on the mesial side and one on the distal side.Three canal orifices were found: mesiobuccal, mesiolingual, and distal. A working length radiograph was taken with a #15 file in the canal and it was confirmed using radiograph (Fig.1.3.). Biomechanical preparation of pulp chamber was achieved by circumferential filing with ISO K files of size # 25 in all canals followed by further shaping using hero shapers files (25(6%) for distal canal and 20(6%) for mesial canals) . Canals were irrigated with 3% sodium hypochlorite and normal saline. After thorough cleaning, canals were dried using paper points. Master cone selection was done and was confirmed with IOPA radiograph (Fig.1.4.). AH plus root canal sealer (Dentsply, Malifer) was then applied using a # 20 reamer along the canal walls. Obturation of the canals were done using GP cones and AH plus sealer with lateral compaction technique in the mesial and distal canal (Fig.1.5.). After that, the elongated pulp chamber was obturated by thermo plasticized Gutta percha using OBTURA- 2 system (Sybron Endo).The final radiograph confirmed a well condensed filling of the canals (Fig.1.6.).
Similar procedure was done for right maxillary first molar.After access opening and thorough cleaning at the furcation area, three canal orifices were found: mesiobuccal, distobuccal, and palatal. A working length radiograph was taken with a #15 file in the canal and it was confirmed using radiograph (Fig.2.1). Biomechanical preparation of pulp chamber was achieved by circumferential filing with ISO K files of size # 25 in all canals followed by further shaping using protaper files (F4 for distal canal and F3 formesial canals). Canals were irrigated with 2.5% sodium hypochlorite and normal saline. After thorough cleaning, canals were dried using paper points. Master cone selection was done and was confirmed with IOPA radiograph (Fig.2.2.). AH plus root canal sealer (Dentsply, Malifer) was then applied using a # 20 reamer along the canal walls. Obturation of the canals were done using GP cones and AH plus sealer with conventional lateral compaction technique. After that, the elongated pulp chamber was obturated by thermo plasticized Gutta percha using OBTURA- 2(Sybron Endo) (Fig.2.3). The final radiograph confirmed a well condensed filling of the canals (Fig.2.4).
 | Fig 1.3 – Working Length Radiograph – 36
|
 | Fig 1.4 – Master Cone Radiograph – 36
|
 | Fig 1.5 - Lateral Compaction Radiograph – 36
|
 | Fig 1.6 – Final Obturation Radiograph – 36
|
 | Fig 2.1 – Working Length Radiograph – 16
|
 | Fig 2.2 – Master Cone Radiograph – 16
|
 | Fig 2.3 - Lateral Compaction Radiograph – 16
|
 | Fig 2.4 – Final Obturation Radiograph – 16
|
Discussion
Taurodontism is a dental anomaly characterized by large pulp chambers and short roots. Roots often bifurcate or trifurcate at a low level. They are thought to result from failure of the Hertwig’s epithelial root sheath to invaginate at the proper time[8]. The most frequently affected teeth are the molars. Clinically the taurodont crown has normal form, structure, color and texture; so can only be diagnosed by radiographs.Taurodontism is predominantly found in molars but alsohas been seen in premolars, mandibular canines andincisors [9],[10].
In 1928, Shaw classified the subtypes of thiscondition as hypotaurodontism, mesotaurodontism andhypertaurodontism based on the relative displacement ofthe floor of the pulp chamber. This subjective, arbitraryclassification led normal teeth to be misdiagnosed astaurodontism. Shifman and Chanannel proposed an index tocalculate the degree of taurodontism. According to this index,taurodontism is present if the distance from the lowest pointat the occlusal end of pulp chamber to highest point at theapical end of the chamber divided by distance from occlusalend of pulpchamber to the apex and multiplied by 100 is 20or above (Hypotaurodontism TI 20-30, Mesotaurodontism TI 30-40 and Hypertaurodontism TI 40-75). Taurodontism canalso be determined if the distance from the highest point ofthe pulp chamber floor to the cemento enamel junction ismore than 2.5 mm.[6],[7]
A taurodont tooth shows wide variation in the size of the pulp chamber, varying degrees of obliteration and canal configuration, apically positioned canal orifices.
Therefore, root canal treatment becomes a challenge.[11], [12] Taurodontism is associated with several developmental syndromes and anomalies including amelogenesisimperfecta, Down’s syndrome, ectodermal disturbance,Klinefelter syndrome, tricho-dento-osseous syndrome, Mohr syndrome, Wolf-Hirschhorn syndrome and Lowesyndrome.[5]
Endodontic treatment in taurodontism teeth has been described as a complex and difficult procedure. Pulp therapy for taurodonts is a challenging treatment, with increased incidence of hemorrhage during access opening which may be mistaken for perforation.Because of the complexity of the root canal anatomy and proximity of buccal orifices, complete filling of the root canal system in taurodont teeth is challenging. A modified filling technique, which consists of combined lateral compaction in the apical region with vertical compaction of the elongated pulp chamber, has been proposed.[11]
Another endodontic challenge related to taurodont teethis intentional replantation. The extraction of a taurodonttooth is usually complicated because of the dilation of theroots in the apical third.[13] In contrast; it is also believedthat because of its large body, little surface area of ataurodont tooth is embedded in the alveolus. This featurewould make extraction less difficult as long as the rootsare not widely divergent.[14]
Conclusion
Although taurodontism are of rare occurrence, clinicianshould be aware of the complex canal system for it successfulendodontic treatment. Sometimes its discovery may help todisclose systemic conditions as well.
References
1. Keith A,Problems related to the teeth of the earlier forms of prehistoric man.Proc R Soc Med 1913;6:103-10.
2. Jafarzadeh H, Azarpazhooh A, Mayhall JT: Taurodontism: a review of the condition and endodontic treatment challenges. International EndodonticJournal, 2008 ;41(5):375-388.
3. Manjunatha BS, Kovvuru SK. Taurodontism- a review on its etiology, prevalence and clinical considerations. J ClinExp Dent2010;2:e187-90.
4. Hamner JE, Witkop CJ Jr, Metro PS. Taurodontism: Report of case. Oral Surg Oral Med Oral Pathol 1964;18:409-18.
5. Joseph M (2008) Endodontic treatment in three taurodontic teeth associated with 48, XXXY Klinefilter syndrome: a review and case report. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 105, 670-677.
6. Shaw JC. Taurodont teeth in South African races. J Anat 1928;62:476-98.
7. Shifman A, Chanannel I. Prevalence of taurodontism found in radiographic dental examination of 1200 young adult Israeli patients. Community Dent Oral Epidemiol 1978;6:200-3.
8. 8.Bhaskar SN (2001) Orban’s oral histology and embryology. 11th ed, CV Mosby, St Louis, 41-44.
9. Parolia A, Khosla M, Kundabala M. Endodontic management of hypo-,meso-, and hypertaurodontism: Case reports. AustEndod J 2012:38:36-41.
10. Bharathi R, Chandra A, Tikku AP, Wadhwani KK. ‘Taurodontism’ an endodontic challenge: A case report. J Oral Sci 2009;51:471-4.
11. Tsesis I, Shifman A, Kaufman AY (2003) Taurodontism: an endodontic challenge: report of a case. J Endod 29, 353-355.
12. Rao A, Arathi R (2006) Taurodontism of deciduous and permanent molars: report of two cases. J IndianSocPedodPrev Dent 24, 42-44.
13. Yeh SC, Hsu TY (1999) Endodontic treatment of taurodontism with Klinefelter’s syndrome: a case report. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 88, 612-615.
14. Durr DP, Campos CA, Ayers CS (1980) Clinical significance of taurodontism. J Am Dent Assoc 100, 378-381.
|
|
|
|
|
|
|