Introduction:
Supernumerary teeth may be defined as any teeth or tooth substance in excess of the usual configuration of twenty deciduous, and thirty-two permanent teeth. These extra teeth are termed as supernumerary teeth. They can be seen in almost any region of the dental arch.[1] The supernumerary teeth may occur in both dentitions, but they are more frequently seen in the permanent dentition with the prevalence range of 0.1-3.4%.[2] The prevalence of supernumerary teeth ranges from 0.8 to 2.1% in deciduous and permanent dentition, respectively.[3] Males are affected approximately twice compared to females with respect to permanent dentition.[4] Etiology of development of supernumerary teeth is not clear. It may be due to dichotomy of the tooth bud.[5] or due to hyper activity theory, suggesting that they are formed as a result of local, independent, conditioned hyperactivity of dental lamina.[6] The supernumerary teeth may be single, multiple, unilateral or bilateral, erupted or unerupted and in one or both jaws. Multiple supernumerary teeth are rare in individuals with no other associated diseases or syndromes.[7] Multiple supernumerary teeth are usually associated with conditions such as cleft lip and palate or syndromes like cleidocranial dysplasia and Gardner's syndrome. Cases involving one or two supernumerary teeth most commonly involve the anterior maxilla, followed by mandibular premolar region.[8] When multiple supernumerary teeth are present (>5) the most common site is mandibular premolars.[9]
Classification of supernumerary teeth may be on the basis of position or form.[1], [8]
Positional variations include:
1. Mesiodens - present in the incisor region and is the most common finding.[10]
2. Paramolars - present beside a molar.
3. Disto-molars - present distal to the last molar.
Based on the shape they can be of 4 types:
1. Conical: peg shaped teeth.
2. Tuberculate: made of more than one cusp or tubercle. They are barrel shaped, usually invaginated. Rudimentary defines teeth of abnormal shape and smaller size, including conical, tuberculate and molariform.
3. Supplemental: the supplemental supernumerary refers to a duplication of teeth in the normal series and is found at the end of a tooth series. The most common supplemental tooth is the permanent maxillary lateral incisor, but supplemental premolars and molars also occur.[2], [11], [12]
4. Odontome: is the fourth category of supernumerary tooth. However, this category is not universally accepted. The supernumerary teeth can cause problems for the eruption and alignment of normal dentition. Associated problems can range from failure of eruption, displacement, crowding, adjacent teeth root resorption, formation of dentigerous cyst or they can be just asymptomatic.[1]
Management of Supernumeraries:
Treatment depends on the type and position of the supernumerary tooth and its effect on adjacent teeth. The management of a supernumerary tooth should form part of a comprehensive treatment plan and should not be considered in isolation.
Indications for Removal of the supernumerary teeth are when:
-
Central incisor eruption has been delayed or inhibited
-
Altered eruption or displacement of central incisors is evident
-
When there is associated pathology
-
Active orthodontic alignment of an incisor in close proximity to the supernumerary is envisaged
-
Its presence would compromise secondary alveolar bone grafting in cleft lip and palate patients;
-
When tooth is present in bone designated for implant placement
-
Spontaneous eruption of the supernumerary has occurred.
Indications for Monitoring Without Supernumerary Removal:
-
Extraction is not always the treatment of choice. They may be monitored without removal when:
-
Satisfactory eruption of related teeth has occurred.
-
No active orthodontic treatment is desired.
-
When there is no associated pathology.
-
Removal would prejudice the vitality of the adjacent teeth
Case Reports:
Case: 1.
A 9 years old boy reported to the department of Pedodontics and preventive dentistry with chief complaint of an extra tooth in his upper front region. Intra oral examination revealed a partially erupted mesiodens between his 11 and 21 towards palatal side (Figure 1 a). This was confirmed by taking occlusal radiograph (Figure 1 b). So the treatment was aimed at extraction of mesiodens (Figure 1 c) and wait for the self alignment of 21 from lip pressure which was slightly labially placed, otherwise teeth were well aligned.
 | (Fig. 1, A) An Intraoral View Showing Mesiodens
 |
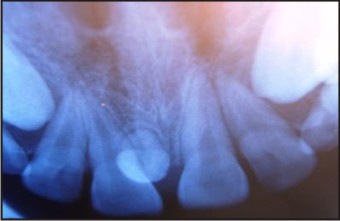 | (Fig. 1, B) An Upper Anterior Occlusal Radiograph Showing Mesiodens
|
 | (Fig. 1, C) Extraction Of The Tooth Done Under Local Anesthesia
|
Case: 2.
Similarly, a 7 years old boy reported with his parents having chief complaint of unusual shaped tooth in his upper front region. Intra oral examination revealed a partially erupted mesiodens in the midline (Figure 2 a). This was confirmed by taking orthopantomogram (OPG) and to rule the possibilities of other unerupted supernumeries (Figure 2 b). So the treatment was also aimed at extraction of mesiodens (Figure 2 c & d) and wait for the eruption11 and 21.
 | (Fig. 2, A) An Intraoral Radiograph Showing Erupted Mesiodens
|
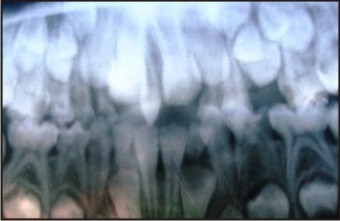 | (Fig. 2, B) An Orthopantomogram Showing The Presence Of Mesiodens
|
 | (Fig. 2, C) An Intraoral View After Removal Of The Tooth
|
 | (Fig. 2, D) Photograph Of The Extracted Mesiodens
|
Case: 3.
Another 71/2 year old child reported with his parents having chief complaint of unusual shaped tooth in his upper front region. Intra oral examination revealed a trabicular type of mesiodens (Figure 3 a). This was confirmed by taking occlusal radiograph and to rule the possibilities of other unerupted supernumeries. So the treatment was also aimed at extraction of mesiodens (Figure 3 b & c) and wait for the eruption 11.
 | (Fig. 3, A) An Intraoral Photograph Showing Eruption Of Trabicular Type Of Mesiodens
|
 | (Fig. 3, B) An Intraoral View After Removal Of The Tooth
|
 | (Fig. 3, C) Extraction Of The Tooth Done Under Local Anesthesia
|
Case: 4.
An 8 years old child visited the department along with his parents for the correction of his upper front teeth. An intraoral examination showed partial healed socket after extraction of erupted tooth (mesiodens) which was done by general dentist (Figure 4 a). As his 11 was severely rotated, so panoramic and occlusal radiographs were advised to rule out the possibilities of other impacted teeth. After reviewing the radiographs an inverted mesiodens was found to be present (Figure 4 b and c), for which we planned to remove and a comprehensive orthodontic treatment was advised for more stable results (Figure 4 d).
 | (Fig. 4, A) An Intraoral View Showing Partial Healed Socket After Extraction Of Erupted Mesiodens
|
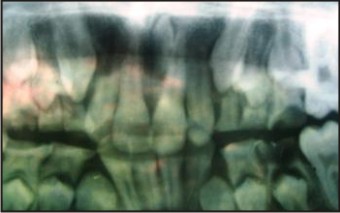 | (Fig. 4, B) An Orthopantomogram Of Same Patient Showing An Inverted Mesiodens
|
 | (Fig. 4, C) An Upper Anterior Occlusal Showing Inverted Mesiodens
|
 | (Fig. 4, D) Extraction Of The Tooth Done Under Local Anesthesia
|
Case: 5.
Almost similar case reported like above with rotation of 21 (Figure 5 a), so panoramic radiograph was advised to rule out the possibilities of impacted teeth. After reviewing the radiographs a mesiodens was found to be present along the incisive canal with slight bulge on the palatal side so a flap was raised from the same side and tooth was extracted followed by suture placement (Figure 5 b, c & d) and further orthodontic treatment was advised for correction of rotation of 21.
 | (Fig. 5, A) Pre-operative Intraoral Photograph
|
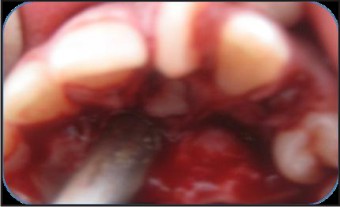 | (Fig. 5, B) Palatal Flap Raised Andtooth Visible In The Socket
|
 | (Fig. 5, C) Extraction Done Under Local Anaesthesia
|
 | Suture Placed After Completion Of Surgery
|
Discussion:
Clinical and radiographic identification of all the teeth is very important for a good treatment planning. It may be difficult to formulate an ideal treatment plan for all cases with supernumerary teeth. But an effort can definitely be made. Treatment may vary from just extraction of supernumerary teeth or extraction followed by orthodontic correction to establish a good occlusion. In the present cases, it was decided to extract the erupted and unerupted supernumerary teeth. Both conical and tuberculate types of supernumerary teeth were found predominantly in the anterior maxillary region. Early diagnosis and intervention is important to minimize the risk of complications and to obtain reasonable alignment and occlusal relationship.[13]
References:
1. Sharer WG, Hine MK, Levy BM. A textbook of oral pathology. 4th ed. Philadelphia: WB Saunders Co, 1983:47-50.
2. Primosch RE. Anterior supernumerary teeth. Assessment and surgical intervention in children. Pediatr Dent 1981; 3:204-15
3. Luten JR. The prevalence of supernumerary teeth in primary and mixed dentitions. ASDC J Dent Child 1967; 34(5) :346-53.
4. Crahnen H, Granath LE. Numerical variations in primary dentition and their correlation with the permanent dentition. Odont Revy 1961; 12:348-57.
5. Tay F, Pang A, Yuen S. Unerupted maxillary anterior supernumerary teeth: Report of 204 cases. ASDC J Dent Child 1984;51(4):289-94.
6. Grahnen H, Lindahl B. Supernumerary teeth in the permanent dentition. A frequency study. Odont Revy 1961; 12:290-94.
7. Castillo KL The incidence of mesiodens in children of Hispanic descent. J Pedod 1986; 10:164-68.
8. Castillo KL. Prevalence of mesiodens in a pediatric Hispanic population. ASDC J Dent Child 1988; 55(2):137-38.
9. Jarvinen S, Lehtinen L. Supernumerary and congenially missing primary teeth in Finnish children. Acta Odontol Scand 1981; 39:83-6.
10. Hogstrom A, Anderssson L. Complications related to surgical removal of anterior supernumerary teeth in children. J Dent Child 1987;54:341-3.
11. Rajab LD, Hamdan MA. Supernumerary teeth: Review of the literature and a survey of 152 cases. Int J Paediatr Dent 2002; 12:244-54.
12. Hattab FN, Yassin OM, Rawashdeh MA. Supernumerary teeth: Report of three cases and review of the literature. J Dent Child 1994; 61:382-93.
13. Profitt WR, Fields HW, Sarver DM. Contemporary orthodontics. 4th ed. St Louis: CN Mosby Co; 1986. p. 138, 243.
|