Introduction
Sudden loss of an anterior tooth is a catastrophic event for a patient. Such an incident has a far reaching impact on an individual’s psychology as well as personality. The aesthetic zone of the anterior region can be affected either due to trauma, periodontal disease or endodontic failure[1]. The anterior teeth are the most vulnerable teeth to get injured during any trauma. Among the various dental traumatic injuries avulsion accounts for 0.5 – 16% of all traumatic injuries and is most commonly observed in young adolescents[2]. Although the re-implantation of the avulsed tooth is the preferred treatment of choice but its success rate is very low and also this immediate treatment is mostly not given , that could be either due to lack of dental facilities or deficient awareness regarding immediate dental preventive measures[3]. The important factors to be considered while management of avulsed teeth are conservation, preservation, minimal invasion, patient acceptance and cost[4]. Whether the tooth is removed surgically or lost due to trauma the dentist should consider an immediate means to satisfy the patient’s cosmetic requirements. In today’s era various materials have been introduced that serve as excellent tooth pontic but nothing replaces natural tooth pontic. It offers the benefits of using the right size, shape and color[5]. These pontics can be stabilized with various Fibre reinforced composite fixed prosthesis, an innovative alternative technique to the conventional fixed restorations[6]. This procedure offers a restorative alternative that produces minimally invasive, aesthetic, time saving, easy and cost-effective metal-free tooth replacement[7]. This case report describes a successful immediate replacement of avulsed tooth in an adolescent using preimpregnated fibre-reinforced composite (INTERLIG) with a follow up of 6 months.
Case Report
A nine year old boy reported to the Department of Pedodontics and Preventive Dentistry, PGIDS Rohtak with the history of fall from cycle 3 days back resulting in loss of upper anterior tooth . In the local clinic he was given medication for pain relief and booster dose of Tetanus toxoid. No other necessary dental management could be done due to lack of any dental facility in that peripheral area. Patient’s father was carrying the avulsed tooth in a bottle filled with water; he was concerned about the appearance of his son and wanted some immediate replacement to be done. Health and family history were not significant.
Clinical examination revealed bilaterally symmetrical face with lacerations on the chin. Mouth opening was normal and there was no pain on examination of the temporomandibular joints. Intraoral examination revealed mixed dentition with missing left maxillary permanent central incisor (Fig 1). Occlusion was normal with bilateral Class I molar relationship . Intraoral periapical radiograph was taken to confirm the integrity of alveolar bone. Re-implantation of avulsed tooth was ruled out considering the extra oral dry time. Because of the time constraint and patients parents desire for immediate aesthetics it was decided to use patients own teeth as pontic and splint it to adjacent teeth using fibre reinforced composite (interlig). The avulsed tooth was cleaned and stored in sterile distilled water to avoid dehydration. Impression and photographs were recorded. Length of the natural pontic as needed was determined on the study model using incisal edge of adjacent teeth and gingival margin as reference point. The root was cut from the crown with a carbide bur and then shaped with a flame shaped finishing bur. The coronal pulp chamber was filled with a bonded composite resin and the gingival aspect of the tooth was smoothed and shaped into an ovate pontic design (Fig 2). It was then checked in the edentulous space for proper position and proximal contacts. The patient was satisfied with the trial appearance.
 | Fig 1: Preoperative Photograph Showing Loss Of Upper Left Central Incisor
 |
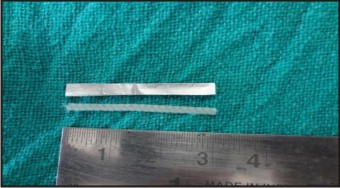
 | Fig 2: Natural Tooth Pontic Made From The Avulsed Tooth
|
Next the lingual surfaces of the abutment teeth were scaled, polished, rinsed and dried. Mesiodistal horizontal grooves were prepared 3mm wide and 0.5mm deep in the enamel of the pontic and the adjacent teeth to accommodate the width and thickness of fibre reinforced composite interlig. The required length of fibre ribbon was measured by placing a template on the lingual surfaces of the teeth, extending from the adjacent left lateral incisor to the right lateral incisor (since the child was in mixed dentition stage the canines were not included for stabilization as they were slightly mobile). A piece of 3mm wide Interlig was taken from its packet using the cotton pliers and cut to an equal length as that of template with the scissors (Fig 3).The natural tooth pontic was first placed in the desired position and stabilized with composite and stainless steel wire onto the adjacent teeth labially. After stabilizing it the grooves of the lingual aspect of the natural tooth pontic and the adjacent teeth were etched with a phosphoric acid etchant (37%) for 15-20 seconds, rinsed with water and dried for 10 sec. A resin adhesive (Single Bond) was applied to the etched enamel surfaces, the tooth preparations, using a disposable brush. Using plastic filling instruments and burnisher, the interlig was embedded into the composite resin starting at the left lateral incisor and moving around the arch to the right lateral incisor (Fig 4). Using a gloved finger wetted with adhesive resin, the ribbon was further pushed into the composite resin so it is covered with composite. It is important that the ribbon be as closely adapted to the lingual surfaces of the teeth as possible. Excess composite resin was removed before light curing. The lingual surfaces were then light cured for 20 seconds. The composite resin was shaped, finished, and polished to remove any excess restorative material and achieve an aesthetic result. This was accomplished with finishing diamonds on a high speed hand piece. The composite resin was further finished using aluminium oxide impregnated silicone composite resin polishing points After complete finishing the splint was checked for occlusion and aesthetic appearance.The final outcome of the procedure left patient highly satisfied with the result (Fig 5). The patient was asked to maintain proper oral hygiene and the limitations of the restoration were informed to him. The patient has been on follow up since 6 months with no problems except for some dietary restrictions.
 | Fig 3: Template Used To Measure The Length Of The Interlig Required
|
 | Fig 4: The Interlig Adapted To The Palatal Aspect Of The Pontic And Adjacent Teeth
|
 | Fig 5: Postoperative Photograph Showing Rehabilitation With Natural Tooth Pontic
|
Discussion
Loss of permanent anterior teeth is an uneventful traumatic experience not only for the child but also for the parents. It compromises mastication, speech and esthetics[8]. It also causes a huge psychological trauma to the child. At present there is no standardized treatment protocol for management of avulsed permanent anterior tooth in cases that occur before cessation of growth[9]. Interim removable partial dentures have been one of the treatment modality but the patients compliance to wear the appliance, its maintenance, subject to fracture, irritation to palatal mucosa and also the psychological setback to the patient does not fulfil our goal of restoring the patients health and overall well being[10]. This clinical report describes a simple , conservative , economical and easy method of replacing a single tooth using Fibre Reinforced Composite and patients own tooth as natural pontic. This type of prosthesis has been referred to as “resin bonded fibre reinforced composite fixed partial denture”. This can be done using two approaches: one is the conventional tooth preparation and laboratory based procedures while the other is based on using the fibres in minimally invasive restorations by direct or indirect fabrication. Direct techniques are conservative, cost effective and does not jeopardise the periodontal health of adjacent teeth[11]. This particular design allows for exact repositioning of the coronal part of the extracted tooth in its original intraoral three-dimensional position. This chair side technique does not require laboratory involvement, is non-invasive and reversible, so that all traditional treatment options for single tooth replacement remain open.[12]
With the introduction of bondable poly ethylene and glass woven fibres, many of the problems with older types of reinforcement were solved[13] and splinting teeth with reinforcement fibres that can be embedded in composites has gained popularity. Procedures can often be completed in a single appointment. It also has an acceptable strength because of good integration of fibres with the composite resin resulting in clinical longevity. In addition, the appliance can easily be repaired in case of fracture due to wear and tear. Moreover, it meets the patient’s aesthetic expectations.[14]
Conclusion
In recent years the desire expressed by many patients for cosmetic and metal free restoration has lead to the development of better performance and truly aesthetic composite resin. Though this technique has excellent aesthetics, preservation of tooth structure and reduced patient cost, Long-term follow-up of preimpregnated fibre-reinforced composite will be required to prove their success. Further laboratory and long-term clinical evaluations are necessary to determine how durable these restorations will prove to be over longer periods of time.
References
1. Strassler HE. Single visit natural tooth pontic bridge with fiber - reinforcement ribbon. Australasian Dental Practice Sept-Oct 2010;158-66.
2. Prasad KEV, Meisheri DJ , Kumar RN ,Nara A , Mahanthesh T Gururaj G. Single sitting interim fixed prosthesis using natural teeth subsequent to avulsion in a 13 year old child .Annals and essences of dentistry Jul – Sep 2013;Vol. V Issue 3:11-14
3. Kretzschmar JL. The natural tooth pontic: A temporary solution for a difficult esthetic situation. J Am Dent Assoc 2001;132:1552-3.
4. Rudraprasad CA, Nandeeshwa DB. Natural tooth pontic: A temporary immediate provisional for a difficult esthetic situation. J Ind Prosth Soc. 2008;8:122–5.
5. Freilich MA, Karmaker AC, Burstone CJ, Goldberg AJ. Development and clinical applications of a light- polymerized fiber-reinforced composite. Prosthet Dent 1998;80:311-18 .
6. Mishra N. Single visit natural tooth Pontic Bridge using fibre reinforced composite – A clinical report. Clinical dentistry, Mumbai January 2013; 23-27.
7. Goel D and Goel GK .Restoring Aesthetics after Anterior Tooth Loss for a Five-Year-Old Child: Natural Tooth Pontic Fibre Reinforced Prosthesis Case Reports in Dentistry Volume 2013, Article ID 215816,1-3.
8. Ulusoy AT, Cehreli ZC. Provisional use of a natural tooth crown following failure of replantation: A case report. Dental Traumatology 2008; 24: 96–9.
9. Daly CG, Wilkinson EJ. Use of patient's natural crown as the pontic in a composite resin-retained temporary bridge. Aust Dent J 1983; 28: 301–3.
10. Ashley M, Holden V. An immediate adhesive bridge using the natural tooth. Br Dent J 1998; 184:18–20.
11. Gupta S, Nikhil V, Gupta S, Verma M. Conservative bridge with natural tooth pontic: a case report. Int journal of clinical dental sciences: 2011:2(2):58-64
12. Dimaczek B, Kern M .Long-term provisional rehabilitation of function and aesthetics using an extracted tooth with the immediate bonding technique. Quintessence Int 2008; 39: 283-8
13. Karbhari VM, Dolgopolski A. Transition between microbrittle and micro-ductile material behaviour during FCP in short fibre reinforced composite.Int J fatigue 1990;12: 51-61.
14. Karman AI, Kir N, Belli S . Four applications of reinforced polyethylene fibre material in orthodontic practice. Am J Orthod Dentofac Orthop 2002; 121:650-54.
|