INTRODUCTION
Periodontal disease belongs to a group of inflammatory disorder whose pathogenesis is not well defined, although it is known that the interaction of host defense mechanisms and etiologic agents is an important determinate of the
onset and progression of the disease. There is well documented evidence that bacteria and their products found in dental plaque comprise the primary etiologic agents responsible for periodontal disease1,2,3.
The primary aim of non surgical as well as surgical treatment regimen is the removal of etiologic factor (i.e. plaque and calculus). Non surgical therapy i.e. scaling and root planing may not always result in the complete elimination of
etiologic factor because of poor access to the base of deep periodontal pocket and anatomical complexities which may occasionally limit the efficiency of root planing. It has also been suggested that residual bacteria in the dentinal
tubules and soft tissues may repopulate the scaled teeth4.
Tetracyclines have been used extensively in the treatment of periodontal disease since many years. Tetracyclines are semi-synthetic chemotherapeutic agents which are bacteriostatic in action and hence are effective against rapidly
multiplying bacteria. Tetracycline and its derivatives have been used systemically as well as locally in the treatment of periodontal disease. Local drug delivery avoids most of the problems associated with systemic therapy by limiting the
drug to its target site with little or no systemic uptake. Tetracycline have been incorporated into a variety of delivery systems (non resorbable or bio resorbable) for insertion into periodontal pockets. These include hollow fibers (Goodson et al 1979) ethylene vinyl acetate copolymer fibers (Goodson et al 1983), ethyl cellulose fibers (Friedman and
Golomb 1982), acrylic strips (Addy et al 1982), collagen preparations (Minabe et al 1989) and hydroxypropylcelluslose films (Noguchi et al 1984)5. Recently , new biodegradable local drug delivery system, Periodontal Plus ABTM (Advanced Biotech Products, Chennai, India) i.e. tetracycline impregnated fibrillar collagen that contains 25 mg pure fibrillar collagen containing approximately 2mg of evenly impregnated tetracycline HCI, has been introduced for the treatment of gingival and periodontal diseases. The present three months study was designed o clinically compare the efficacy of tetracycline from modified collagen matrix used as combination therapy with scaling and root planing alone in the treatment of chronic periodontitis.
MATERIALS & METHODS
A total of 35 human subjects comprising of both sexes (Male : Female = 16:19), aged between 5to 60 years were selected from the Out Patient Department of Periodontics at the D.A.V. (C) Dental College and Hospital, Yamunanagar,
Haryana (India). All the 35 subjects completed the 3 month follow up study
STUDY POPULATION:
· INCLUSION CRITERIA
1. Patients who had not undergone any surgical or non-surgical periodontal therapy in the past 6 months.
2. Patients who had not taken antibiotic therapy in the past 6 month.
3. Patients able to follow verbal or written oral hygiene instructions.
4. Patients having 2 nonadjacent teeth separated by atleast 1 tooth with e” 5mm periodontal pocket that bleed on probing at the initial visit.
EXCLUSION CRITERIA
1. Patients with a history of using anti- microbial mouthrinses within 2 months of the baseline visit or on routine basis.
2. Patients having history of allergy to tetracycline or cyanoacrylate adhesive.
3. Pregnant woman or nursing mothers.
4. Patients with periodontal packets in which the depth of the pockets corresponded to the apex of the tooth as in probable endodontic –periodontic conditions.
5. Medically compromised patients.
6. Teeth with furcation involvements.35 subjects with a total of 70 sites were selected. The selected sites were randomly divided into test group and control group.
· Test Group included 35 sites treated with local drug delivery and scaling and root planing.
· Control Group included 35 sites treated with scaling and root planing alone (without local drug delivery).
CLINICAL PARAMETERS RECORDED
· Plaque Index (Silness and Loe 1964)6 at baseline, 1month, 2months and 3months post therapy.
· Gingival Index (Loe and Silness 1963) 7 at baseline, 1month, 2months and 3months post therapy.
· Probing Depth measurement from gingival margin to base of pocket using William’s graduated probe at baseline, 1month, 2months and 3months post therapy.
· Clinical Attachment Level measurement from cemento-enamel junction as a reference point to the base of pocket with William’s graduated probe at baseline, 1month, 2months and 3months post therapy.
STATISTICAL METHODS:
The baseline, 1month, 2months and 3months value were compared for changes that occurred over time i.e. changes in plaque index, gingival index, probing depth reduction and clinical attachment gain. Probabilities less than 0.05 (p < 0.05) were considered significant. Probabilities less then 0.001(p < 0.05) were considered highly significant. The paired t- test
and student t-test were utilized to evaluate and establish differences between baseline and 1, 2 and 3 months values of test and control sites.
TETRACYCLINE IMPREGNATED
FIBRILLAR COLLAGEN:
This product consists of 25mg of pure fibrillar Type-I collagen containing approximately 2mg of evenly impregnated Tetracycline HCI, USP/ IP. It is available as a strip containing four individually packed and separable sterile product
packs. Just before placement, fibers were soaked with saline in a sterile dappen dish. Soaked fiberwere placed at the prepared site and gently pushed inside the pocket, so that the material fills the depths and curves of the pocket. Hand pressure was applied for just a few minutes to encourage hemostasis and initial setting of the material inside the pocket. The site was sealed with cyanoacrylate adhesive to prevent ingress of oral fluids.
POST TREATMENT INSTRUCTIONS:
1. Avoid chewing hard or sticky food.
2. No flossing on the treated site.
3. Do not disturb the area with tongue, finger or tooth pick.
4. To report immediately if the material is dislodged before the scheduled recall visit or if pain, swelling or any other complication occurs.
RESULTS
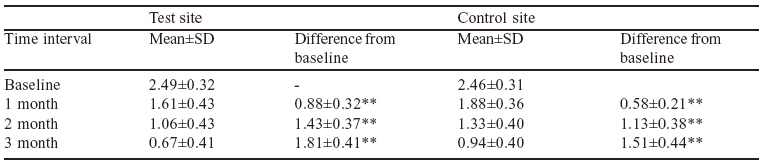
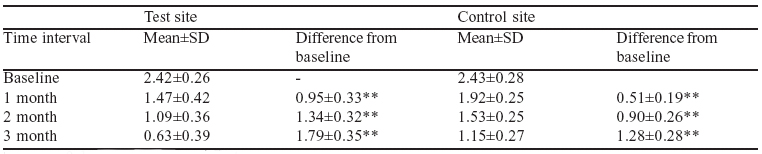
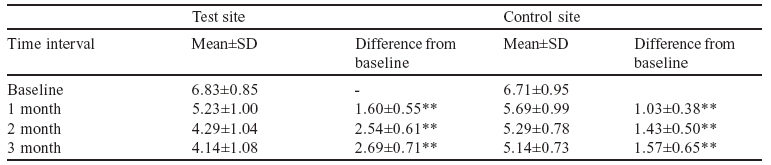
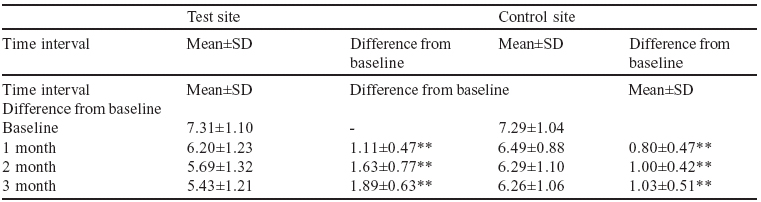
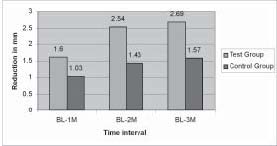
The clinical finding at baseline, 1 month, 2 months and 3 months post operative are shown in table 1, 2, 3 and 4. At the start there was no significant difference between both treatment group for the plaque index, gingival index, probing ocket depth and Clinical attachment level (p d” 0.001). Table 3 and Graph 1 shows a gradual reduction in probing pocket depth both for test and control group, with more reduction in test group as compared to control group. Similarly more gain in clinical attachment level in the test group as compared to control group is evident from table 4 and Graph 2.
DISCUSSION
One essential goal of current periodontal therapy is successful management of the suspected bacterial pathogens to the extent that destruction of the periodontium is arrested. A number of different non-surgical and surgical therapies have been successful in achieving this goal. Mechanical debridement with or without surgical manipulations, to disrupt the subgingival flora and to provide clean , smooth and biological compatible roots surfaces, had been the therapy to treat periodontal diseases till the early 1970’s. Mechanical therapy may however fail to eliminate the pathogenic bacteria because of their location within gingival tissues or in other areas inaccessible to periodontal instruments8.
The present study was designated to access the clinical efficiency of tetracycline impregnated collagen fibers by demonstrating then changes in plaque index and gingival index, changes in probing pocket depth and clinical ttachment
level. A total of 35 patients (Male: Female=16:19) were enrolled in this study. Two interproximal sites with pocket depth e” 5mm were selected in each
patient in different quadrants. Possible side effect of therapy including slight discomfort and gingival redness were evaluated. No treatment related adverse effects were observed in any patient. Garret et at 19999 also reported that treatment emergent adverse events constituted d” 1% of the entire study population with 0.2% of them showing allergic response. In the present study significant reduction in plaque score from baseline to 3 months for both treatment group (p 0.001) was observed Similar observation were made by Minabe et al 199110, Heijl et al 199111, Mehta et. Al 20005 and Frisen et al 200212 who found low levels of plaque index scores in this study from baseline could be due to
a greater attention to oral hygiene practice by all selected participants throughout the study. Similarly gingival index also showed
significant reduction in scores from baseline to 3 months for both treatment groups. Minabe at al 199110 and Mehta et al 20005 observed low levels of gingival index scores throughout the period of study. Control of plaque and gingivitis is important in clinical studies because both vary in their association with periodontitis and both affect measured response to therapy, in this study, the reduction in plaque and gingival index may be due to thorough oral prophylaxis and proper home care by patients. Since increased probing depth and loss of clinical attachment are pathogonomonic for
periodontitis, hence pocket probing is a crucial and mandatory procedure in diagnosing periodontitis and evaluating the success of periodontal therapy. In the present study intra group observation showed highly significant (p < 0.001) reduction in probing depth from baseline to 3 months in both group.
On comparison, statistically significant differences was observed from baseline to 3 months between scaling and root planing alone and combination therapy. The results are consistent with the findings of Goodson et al 1991 13, Minabe
at al 1991 10, Newman et al 1994 14, Tonetti et al 1991 15, & Mehta et al 20005. These finding are in contrast with the result of Drisko et al (1995)16 who observed no significant difference among the different regimens at any point in time. This could be attributed to the fact, that in Drisko et al 1995 16 study tetracycline fibers were placed in non root planed sites and benefit of mechanical debridement was not obtained.
Newman et al 199414 quoted that patients tend to have approximately 1 mm reduction of probing depth on average, but in some cases, can have more dramatic effects, such as 2mm or greater. It was similar to the findings of this study.
Goodson et al 199113 also observed that probing depth reduction was higher in combination therapy than scaled sites. Heijl et al 199111 in their comparative study also observed that there was significant pocket depth reduction in the combination therapy than scaling root planing alone.
A significant gain in clinical attachment level was also obtained from baseline to 3 months in both the treated sites (p < 0.001) difference was observation were similar to that of Goodson et al 199113, Heijl et al 199111, Minabe et al 199110,
Newman et al 199114, Drisko et al 199516, Kinane and radvar 199917. On comparison, highly significant (p < 0.001)
difference was observed between combination therapy and scaling and root planing alone. This finding is similar to that of Goodson et al 199113, Minabe et al 199110, and Newman et al 199414. Minabe et al 199110, found gain of clinical
attachment level around 2mm, and suggested that the local application of antibiotic using a local drug delivery in combination with root debridement may contribute to clinical attachment gain. The finding of the study is in contrast with
those of Drisko et al 199516 who found no significant among the different regimens at any time point. This could be due to reason as mentioned earlier.
The higher efficacy of the modified collagen matrix and tetracycline over scaling and root planing, could be attributed to the availability of a modified collagen matrix to accelerate tissue restructuring, the sustained delivery of a potent
drug (tetracycline) that eradicated periodontopathic microorganisms and the ability of tetracycline to inhibit bacterial collagenases.
The reduction of probing depth and gain of clinical attachment were significant in all treatment groups. These improvements might simply reflect a change in tissue composition of periodontal tissues, rather than a true gain of new attachment.
Armitage et al. and Spray et. al. have found that inflammation of the gingival tissue has a significant influence on the degree of probe penetration5. Improved gingival health may have contributed to the observed reduction of probing depth, presumably by decreasing the edematous swelling of the marginal gingiva and / or by decreasing the penetrability of tissue by the probe as a result of an increase of collagen content. The crux of the present study clearly shows
that mechanical debridement and locally delivered tetracycline work by two different mechanisms. Scaling and root planing removes some amount of bacteria without providing bactericidal activity whereas tetracycline does not remove any calculus deposits. Hence neither is the ideal control for the other. Together, locally delivered tetracycline
therapy has a specific purpose of controlling localized infection, and scaling and root planning to remove calculus and other deposits, providing added benefits and the rate of new lesion formation is also decreased by the combination
therapy.
CONCLUSION:
1. Application of the tetracycline in modified collagen matrix following scaling and root planing might be beneficial in treatment of chronic adult periodontitis and improving periodontal parameters for 3 months duration. 2. Though the local drug delivery system used in the study is the safe and effective treatment modality, further clinical and microbiological
studies are required to determine the effect of this treatment modality over long period.
Inspite of the proven additive benefits, the availability and cost associated with various controlled delivery devices (EVA fibers) have so far limited the application of tetracycline fibers. As this material is relatively cost effective and biodegradable, its use can be expanded in general population.
REFERENCES
1. Listgarten MA et al Role of dental plaque in gingivitis and periodontitis. J Clin Periodontol 1988; 485-487.
2. Haffajee AD, Socransky SS Microbiological etiological agents of destructive periodontal disease. Periodontology
2000, 1994; 5: 78-111.
3. Socransky SS, Haffajee AD The bacterial etiology of destructive periodontal disease: Current concepts. J Periodontol
1992; 63: 322-331.
4. Goodson JM et al Antimicrobial strategies for treatment of periodontal disease. Periodontology 2000. 1994; 5: 142-168.
5. Mehta DS et al A comparative assessment of the efficacy of tetracycline fibre therapy and phase 1 therapy in the treatment of chronic adult periodontitis. JIDA 2000; 71:207-211.
6. Silness P, Loe H Periodontal disease in pregnancy. Acta Odontol Scand 1964; 22: 121.
7. Loe H, Silness J Periodontal disease in pregnancy. Acta Odontol Scand 1963; 21: 533.
8. Slots J, Rams TE Antibiotics in periodontal therapy: Advantages and disadvantages. J Clin Periodontol 1990; 17:
479-495.
9 Garrett S, Johnson L, Drisko CH Two multicenter studies evaluating locally delivered doxycycline hyclate, placebo
control, oral hygiene and scaling and root planing in the treatment of periodontitis. J Periodontol 1999; 70: 490-503.
10. Minabe M et al Therapeutic effects of combined treatment using tetracycline immobilized collagen film and root planing in periodontal furcation pockets. J Clin Periodontol 1991; 18: 287-290.
11. Heijl L, Dahlen G, Sundin Y, Wenander A, Goodson J A four quadrant comparative study of periodontal treatment using tetracycline containing drug delivery fibres and scaling. J Clin Periodontol 1991; 111-116.
12. Frisen LR et al Controlled local delivery of tetracycline with polymer strips in the treatment of periodontitis. J Periodontol 2002; 73: 13-19.
13. Goodson JM et al Multicenter evaluation of tetracycline therapy (ii). Clinical response. J Periodontol Res 1991; 26:371-379.
14. Newman M et al A 6 month multicenter evaluation of adjunctive tetracycline fiber therapy used in conjunction with
scaling and root planing in maintenance patients: clinical results.J Periodontol 1994; 65: 685-691.
15. Tonetti M et al Principle and clinical applications of periodontal controlled drug delivery with tetracycline fibers.
Int J Peridont Rest Dent 1994; 14: 421-435.
16. Drisko C et al Evaluation of periodontal treatments using controlled release tetracycline fibers: clinical response. J
Periodontol 1995; 66: 692-699.
17. Kinane DF et al A 6 month comparison of the three periodontal local antimicrobial therapies in persistent periodontal pockets. J Periodontol 1999; 70: 1-7.
Table 1 : Mean Values Of Plaque Index At Baseline, 1 Month, 2 Months And 3 Months Post Operatively (Test Site & Control Site)
** = Pd” 0.001 – Highly Significant
Table 2 : Mean Values Of Gingival Index At Baseline, 1 Month, 2 Months And 3 Months Post Operatively (Test Site & Control Site)
** = Pd” 0.001 – Highly Significant
Table 3 : Mean Values Of Pocket Depth At Baseline, 1 Month, 2 Months And 3 Months Post Operatively (Test Site & Control Site)
** = Pd” 0.001 – Highly Significant
Table 4 : Mean Values Of Clinical Attachment Level At Baseline, 1 Month, 2 Months And 3 Months Post Operatively (Test Site & Control Site)
** = Pd” 0.001 – Highly Significant
GRAPH 1: MEAN POCKET DEPTH REDUCTION AT DIFFERENT TIME INTERVAL
GRAPH 2: MEAN CLINICAL ATTACHMENT GAIN AT DIFFERENT TIME INTERVAL
|