INTRODUCTION
The term occlusal interference is generally understood to denote an undesirable contact between some aspect of the maxillary and mandibular dentitions, with a consequent disruption of fluid mandibular closure into maximum intercuspation, or unhindered movement of the mandible in protrusive or lateral excursive movements. Anterior interferences have been defind as : An occlusal interference on the anterior teeth, identified during unforced closure of the mandible, sometimes associated with a distalizing effect on condylar position. They are seen more commonly in cases with retroclined maxillary incisors and under torque upper central incisors. These interferences may lead to severe attrition of the anterior teeth, anterior spacing, gingival recession or intra capsular derangement of the TMJ. This case report documents the orthodontic and restorative treatment of destructive occlusal wear in the anterior region.
A 34 year old female presented with presented with a single, irregular, reddish, pedunculated 2x2 cms gingival swelling on lingual side w.r.t 47,48 (Fig.1).
CASE REPORT:
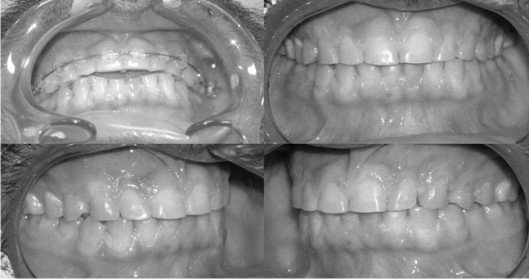
The patient, a 46 year old male reported with a chief complaint of hypersensitivity and attrition of lower front teeth. Excessive incisal wear was noted on the mandibular central incisors.(fig 1) However, there was virtually no discernible wear on the lateral incisors, and it is quite unlikely that the effects of bruxism would be this localized without some other factor being involved. The type of excessive incisal wear noted in this example is an obvious deleterious effect of an anterior interference. The lower left lateral incisor was non vital. Molar relation was class I, over jet was 1mm and overbite was 80%. The oral hygiene was acceptable, the probing depths were normal. Cephalometric examination revealed retroclined maxillary incisors and correctly inclined mandibular incisors. Radiological examination presented no other significant finding.
 | Fig 1
 |
Figure 1: Pre-Treatment photographs of the patient showing retroclined incisors and severe attrition of the mandibular incisors.
TREATMENT
Treatment plan was presented to the patient. The patient was informed regarding orthodontic bite opening procedure, correcting the axial inclination of teeth and establishing a correct interincisal angle and hence the incisal guidance. The patient understood the plan and gave his consent for the orthodontic treatment and restorative procedures.
Endodontic treatment of 32 was performed. A deprogramming splint was fabricated and adjusted for the patient. Patient was comfortable with it in 1 week. He was recalled every two weeks for 2 months. Slight bite opening was observed. Orthodontic treatment was instituted using 018 slot Roth prescription only in the upper dentition. No orthodontic intervention was done in the lower jaw. Alignment and leveling was done with round and later with rectangular 16 x 22 NiTi wires. This resulted in correction of inclination of upper incisors and bite opening. After bite opening with intrusion of maxillary incisors adequate overjet and over bite was achieved with consolidation of the spaces that appeared between the anterior teeth. (Fig 2).
 | Fig 2
|
Figure 2. Photograph showing adequate overjet and over bite achieved to allow restoration of the attrided lower incisors.
Filtek Z 350 (3m Unitek) was used to restore the lower anteriors.(Fig 2). A Hawley’s retainer with anterior bite plane was fabricated and delivered to the patient.
CONCLUSION
The purpose of this article was to introduce the concept of correction anterior interferences before restoring the worn off dentitions and not just restoring the teeth after raising the bite. It is of paramount importance to understand that correct axial inclination of maxillary and mandibular anteriors and not just bite opening will ensure the longevity of the restorations.
REFERENCES
1. Edwards JG. The diastema, the frenum, and the frenectomy. AJO 1997;71:489-500.
2. Giargia M, Lindhe J. Tooth mobility and periodontal disease. J Clin Periodontal 1997;24:785-795.
3. Perrier M, Polson A. The effect of progressive and increasing tooth hypermobility on healthy periodontal supporting tissue. J Periodontol 1982;53:152-157.
4. McNamara JA Jr, Seligman DA, Okeson JP. The relationship of occlusal factors and orthodontic treatment to temporomandibular disorders, in Temporomandibular Disorders and Related Pain Conditions: Progress in Pain Management Research, Vol. 4, p 399.
5. Isberg A, Isacsson G. Tissue reactions of the temporomandibular joint following retrusive guidance of the mandible. J Craniomadibular Practice 1986;4:143-148 |