Introduction
The success of root canal treatment is marked by numerous factors ranging from straight line access cavity preparation to choice of sealer, irrigant and obturating material as well as technique. In the present era of high tech dentistry, various opinions with many innovative concepts and techniques on how to best accomplish the goals of canal debridement, cleaning and shaping and obturation are released daily.
Although the curriculum and guidelines of the undergraduate program are set up with the viewpoint of making students learn the endodontic procedures with optimum knowledge and skills, no protocol is designed in India to gauge the attitude of these graduates when they start working as General Dental Practitoners (GDPs). Little data is available regarding implementation of the standards taught, and on how far the changes in endodontic technique have been incorporated into daily practice by dental health practitioners.
After graduation, dentists work independently in unsupervised dental practices where attitude towards existing treatment standards differs.[1] This difference in attitudes towards endodontic treatmentperformed can lead to the errors that impede the healingprocess.[2] This difference of attitudes towards endodontictreatment can also make it impossible to accomplish theendodontic treatment according to aseptic principles that areessential for the success of endodontic treatment[2].
Variousstudies[2],[3],[4],[5],[6] have been done to evaluate the success andfailure of endodontic treatment, and these studies have shownthat the failure could be significantly higher for those teethwhich are treated by general dentists not by endodontists.[6] From a public health care point of view, the issue of treatment efficiency and cost is also important because resources in the society are limited in a developing nation as ours. Hence they should be directed to the most effective and the most efficient treatment regimen. However, very few data are available about the GDPs approach to endodontic therapy.[7],[8] These studies mention that a majority of GDPs do not conform to established guidelines. Thus keeping in consideration the above findings, a study was planned and conducted to investigate the current opinions of the GDPs in four adjoining states of North India regarding knowledge towards fundamental aspects, materials, methods, and attitudes employed during endodontic treatment by dentists and to compare them to academic standards of treatment and established quality assurance guidelines.
Materials & Methods
Registered dentists in the state of Himachal Pradesh were included in the study. Though only those whose E mail addresses were available in the state dental council records could be reached. Moreover, it was mentioned at the starting of the questionnaire that it was meant strictly for the dentists who are into any kind of practice. The questionnaire was designed to cover all the possible facets of root canal treatment. The prepared questionnaire was electronically mailed to 8550 dentists and information about the standard protocols of root canal treatment was collected. Information ranging from the personal details like gender, nature of professional activity to details of use of instruments, methods of isolation, working length determination, techniques of root canal preparation, root canal irrigants, intracanal medicaments, and methods of root canal obturation was covered in the form of multiple choice questions. The collected data was analyzed by using SPSS 10 computer software to get the results. Simple descriptive analysis was used to get the results as frequencies and percentages.
Results
Out of 8550 questionnaires mailed, 2066 replies were received. However, only 2000 were evaluated as useable as ones with incomplete or wrong markings were excluded thus giving a response rate of around 24% for the study. The results showed that 52% of respondents were General Dental practitioners (GDP) and only 23% were Endodontists. (Table 1) In spite of female dominance in the admission rate to dental colleges in the country, a large percentage of 77% dental practitioners were males. A majority of respondents never used rubber dam (68.5%) with only 182 dentists reportedly using rubber dam always for endodontic treatment. However, 76% of dentists were found using Nickel Titanium Instruments thus reflecting the up gradation in the treatment standards in our nation. 1290 respondents aimed at achieving a working length between 0 and 1mm short of the radiographic apex. About 58% instrumented the canal With a Step Back technique, generally using a combination of different instruments (K File +Hedstrom file). 93% dentists were found using Zinc oxide eugenol as sealer with very less of them opting other ones like metapex or AH plus. Similarly Cavit was the temporary filling material of choice for majority of practitioners. Only 12% of them opted IRM, 16.4% used ZOE, rests all were found using Cavit. Choice of irrigants, intracanal medicament and obturating material is depicted in Figure 2 & 3 respectively.
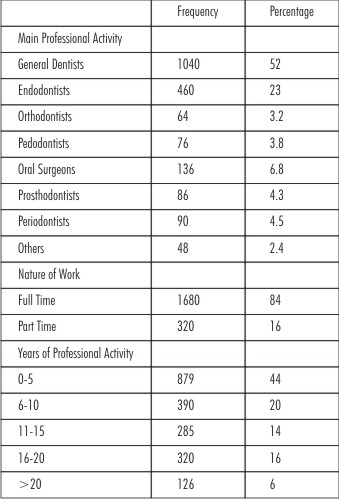 | Table 1 : Demographic & Professional Data Of Respondents
 |
Discussion
The study was carried out with the aim to determine the knowledge of practicing dentists in the state of Himachal Pradesh towards the various aspects of root canal treatment. Email addresses of registered dentists were obtained from the State dental council. The nature and the purpose of the study were explained to the authorities and approval was taken. A self prepared questionnaire was electronically mailed to all dentists. Only 8550 mails could be delivered, out of which 2066 replied thus making response rate of 24% which is comparable to the similar studies done in Belgium[9] and England[10] but less than one carried out by Jenkins et al in 2001.[7]
52% of dental health practitioners in the state were general dentists owing to the high number of Undergraduate seats in dental colleges with very less percentage of students opting for post graduate degree thus reducing the number of specialized practitioners. Majority (77%) of practicing dentists were males in spite of greater rate of female admission in undergraduate program. The finding showed that females give up dentistry as profession after graduation owing to reasons like family burdens or their dependent nature in our country. The saturation of professional souk is well portrayed by the highest number of practicing dentists with the work experience in the range of 0-5 and 6-10 years.
Rubber dam isolation is considered the standard of care in endodontics. Despite its importance, only 9.1% of the total responding dentists in the present study were always using rubber dam and majority of the respondents, that is, 68.5%, were using cotton rolls for isolation during endodontic treatment. In UK,[11] only about a quarter of respondents routinely used rubber dam during root canal therapy; however, in America 59%[8] and in New Zealand 57%[12] of the dentists were using rubber dam routinely in endodontic treatment. In a similar study, conducted in KSA, only 3% of the respondents were using rubber dam as the method of isolation. This lack of use of rubber dam can directly affect the standard of root canal treatment and decrease the success rate. Practitioners may equate rubber dam use with time loss, patient pain, extra cost, frustration and irritation.[13]
The determination of working length is the most crucial step in the endodontic treatment[14]. However, determination of the working length has always been a challenge for the clinician as the point of exit of the root canal in the apical region is highly variable owing to its tortuous anatomy. The optimal working length in teeth with vital pulp appears tobe1-2 mm from the radiographic apex[15]. In the study of Sjogren et al. (1990), it was stated that in cases where the pulp was necrotic and infected, the working length should be chosen within 1mm of the radiographic apex[3]. In the present study, 64.5% dentists used instrumentation levels1mm short of the radiographic apex, independent of the pathology. However, radiographic method has inherent inaccuracies, as the apical foramen is not detectable on radiograph[16]. Electronic apex locator has the advantage of being able to locate the apical foramen[17],[18]. Therefore, it is highly recommended to combine the use of electron apex locator and radiographs to make an efficient and accurate determination of working length.
Majority of the dentists (76%) in the present study were using Nickel Titanium rotary and hand instruments, indicating that new developments are being slowly and gradually being incorporated into practice by the dentists in the state. Step Back technique, generally using a combination of traditional instruments (K File +Hedstrom file) was the method of choice for the instrumentation in about 58% of GDPs. However, this standardized technique of root canal preparation has some disadvantages like overpreparation resulting in elliptically shaped defect at the end-point of preparation[19], which could result in incomplete obturation of the root canal system. Therefore those preparation techniques which involve the early coronal flaring, for example, crown-down technique, should be adopted as they will produce a better shape and enhanced penetration of irrigating solution[20]. But unfortunately in present study, only 7.4% of the dentists were using this technique.
The sodium hypochlorite is recommended as the material of choice for irrigating the root canal system because of its effective antimicrobial and tissue dissolving action[21],[22]. However, unfortunately in the present study, majority (38%) of our respondents were found opting saline as an irrigant of choice. Easy availability, cost effectiveness and the limited use of rubber dam by the practitioners could be among the reasons behind popular use of saline. In a study of Whitten et al. (1996)[8], 79% of the GDPs used sodium hypochlorite as irrigant, whilst in the survey of Whitworth et al. (2000)[11] in UK general dental practice, local anaesthetic solution was the most commonly used endodontic irrigant. Many clinicians prefer dilute concentrations to reduce the potential of sodium hypochlorite to act as an irritant[23].
The main objective of the use of intracanal medicaments is to reduce the number of bacteria, to relieve pain, to reduce inflammation, and to dry the wet canals[24]. In present study, 887 respondents out of 2000 (Figure 1), were using formocresol as intracanal medicament. Formocresol has many adverse effects due to its mutagenicity[25]. Although calcium hydroxide is considered as standard intracanal dressing, only 26.2%of the dentists in the present study were using this followed by Metapex in around 22% cases. The antibacterial and multiple biological properties of calcium hydroxide should be taken into account and its use must be encouraged in place of formocresol[26],[27]. Gatewood et al. reported a decrease in the use of the more classical medicaments, especially camphorated monochloro phenol with exception to the use of formocresol when vital pulp tissue was present[28]. Temporary restorative materials used in endodontics must provide a high quality seal of the access preparation to prevent microbial contamination of the root canal[9]. 71.6% percent of the respondents use Cavit as temporary filling material, which under experimental conditions provided superior resistance tobacterial leakage[29].
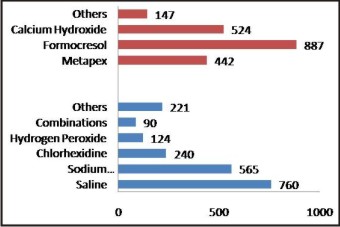 | Figure 1 : Choice Of Intracanal Medicament (Upper Bars) & Irrigant (Lower Bars) Among Respondents
|
According to ESE (1994) guidelines[30], sealers should be biocompatible. A survey in England reported that most private practitioners used non-medicated zinc oxide eugenol root-canal cements whereas the majority of NHS practitioners used one particular medicated sealer, Endomethasone (Septodont, Paris, France)[10]. A very high percentage of 93% in our study was found using ZOE as root canal sealer with negligible no. of dentists opting AH26 (4.2%) and metapex(2.8%).
Root canal obturation with good seal is very crucial step in endodontics to prevent the ingress of microorganisms into already cleaned root canal system. Lateral condensation of gutta percha with sealer is a relatively simple, versatile, universally acknowledged, and most common obturation technique that has produced good results and does not require expensive equipment[31], [32]. In the present study, 57.5% (Figure 2) of the respondents were using lateral condensation technique with a root canal sealer as the root canal obturation technique. In a similar study, the lateral condensation technique with sealer was the most common, that is, 87%, among the surveyed general dental practitioners[31]. Over the years, numerous methods have been advocated to obturate the prepared root-canal system, each with their own claims of ease, efficiency or superiority. In spite of an inundation in obturating materials and techniques in the current market of dental materials, a very small percentage, that is, 2.4% , of the practitioners were using modern obturating techniques like thermo mechanical obturating techniques in the present study.
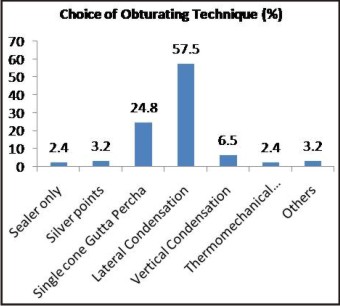 | Figure 2 : Choice Of Obturating Materials Among Respondents
|
Conclusion
Endodontics has always emerged as the most dynamic discipline of dentistry. Advances in materials and techniques have made the root canal treatment the most successful and favorable treatment option in past few decades. The aim of the present study was to assess the quality of practice among the dental health practitioners and their accomplishment towards these standards. The study however showed that endodontic procedures in general practice and quality guidelines differ, especially in the low use of rubber dam and the choice of irrigants and sealers. The results indicated that there is dearth in the knowledge update regarding the instruments, materials and procedures in endodontics. Also the system of referral and specialization practice needs to be incorporated in the system for better quality and results. There should also be conduction of properly structured continuing education courses in endodontics, under the supervision of highly professional endodontic specialists, to meet the demands and needs of general dental practitioners regarding the modern equipment and new techniques in endodontics.
References
1. Iqbal A, Akbar I, Qureshi B, Sghaireen M G, Mahmoud K A. Survey of Standard Protocols for Endodontic Treatment in North of KSA. ISRN Dentistry 2014;Article ID 865780:4 pages.
2. Gorni F.G.M., Gagliani M.M. The outcome of endodontic retreatment: a 2-yr follow-up. Journal of Endodontics 2004; 30(1):1-4.
3. Sjogren U, Hagglund B, Sundqvist G, and Wing K. Factors affecting the long-term results of endodontic treatment. Journal of Endodontics 1990;16(10): 498–504.
4. Eriksen H.M. Endodontology—epidemiologic considerations. Endodontics & Dental traumatology 1991; 7(5): 189-195.
5. European Society of Endodontology. Consensus report of the European Society of Endodontology on quality guidelines for endodontic treatment. International Endodontic Journal 2002; 35: 759–767.
6. Weiger R, Axmann-Krcmar D, Lost C. Prognosis of conventional root canal treatment reconsidered. Endodontics and Dental Traumatology 1998; 14(1): 1-9.
7. Jenkins SM, Hayes SJ, Dummer PM. Astudyof endodontic treatment carried out in dental practice within the UK. International EndodonticJournal 2001;34:16-22.
8. Whitten BH, Gardiner DL, Jeansonne BG, and Lemon RR. Current trends in endodontic treatment: report of a national survey. Journal of the American Dental Association 1996; 127(9): 1333–1341.
9. Slaus G, Bottenberg P. A survey of endodontic practice amongst Flemish dentists. International Endodontic Journal 2002; 35: 759-767.
10. Pitt Ford TR, Stock CJR, Loxley HC, Watson RMG. A survey of endodontics in general practice in England. British Dental Journal 1983; 83: 222-4.
11. Whitworth JM, Seccombe GV, Shoker K, and Steele JG. Use of rubber dam and irrigant selection in UK general dental practice. International Endodontic Journal 2000; 33(5): 435–441.
12. Koshy S and Chandler NP. Use of rubber dam and its association with other endodontic procedures in New Zealand. New Zealand Dental Journal 2002; 98(431): 12–16.
13. Christensen GJ. Using rubber dams to boost quality, quantity of restorative services. The Journal of the American Dental Association 1994; 125(1): 81–82.
14. Ricucci D. Apical limit of root canal instrumentation and obturation, part 1. Literature review. International Endodontic Journal 1998; 31(6): 384–393.
15. Kerekes K, Tronstad L. Long-term results of endodontic treatment performed with a standardized technique. Journal of Endodontics 1979; 5: 83-90.
16. Olson AK, Goerig AC, Cavataio RE, and Luciano J. The ability of the radiograph to determine the location of the apical foramen. International Endodontic Journal 1991; 24(1): 28–35.
17. G. Pagavino G. A SEM study of in vivo accuracy of the root ZX electronic apex locator. Journal of Endodontics 1998; 24(6): 438–441.
18. DeMoor RJG, Hommez GMG, Martens LC, and deBoever JG. Accuracy of four electronic apex locators: an in vitro evaluation. Endodontics & Dental Traumatology 1999; 15(2): 77–82.
19. Weine FS, Kelly RF, and Lio PJ. The effect of preparation procedures on original canal shape and on apical foramen shape. Journal of Endodontics 1975; 1(8): 255–262.
20. Fava LRG. The double-flared technique: an alternative for biomechanical preparation. Journal of Endodontics 1983;9(2): 76–80.
21. Bystrom A and Sundqvist G. Bacteriologic evaluation of the effect of 0.5 percent sodium hypochlorite in endodontic therapy. Oral Surgery Oral Medicine and Oral Pathology 1983; 55(3): 307–312.
22. Wadachi R, Araki K, and Suda H. Effect of calcium hydroxide on the dissolution of soft tissue on the root canal wall. Journal of Endodontics 1998; 24(5): 326–330.
23. Becker GL, Cohen S, Borer R. The sequelae of accidentally injecting sodium hypochlorite beyond the root apex. Oral Surgery 1974; 38: 633-5.
24. Bystrom A, Claesson R, and Sundqvist G. The antibacterial effect of camphorated paramonochlorophenol, camphorated phenol and calcium hydroxide in the treatment of infected root canals. Endodontics & Dental Traumatology 1985; 1(5): 170–175.
25. Block RM, Lewis RD, Hirsch J, Coffey J, and Langeland K. Systemic distribution of [14C]-labeled paraformaldehyde incorporated within formocresol following pulpotomies in dogs. Journal of Endodontics 1983; 9(5): 176–189.
26. Abbott PV. Medicaments: aids to success in endodontics. Part 2. Clinical recommendations. Australian Dental Journal 1990; 35(6): 491–496.
27. Foreman PC and Barnes IE. Review of calcium hydroxide. International Endodontic Journal 1990; 23(6): 283–297.
28. Gatewood RS, Himel VT, Dorn SO. Treatment of the endodontic emergency: a decade later. Journal of Endodontics 1990; 6: 284-91.
29. Beach CW, Calhoun JC, Bramwell JD, Hutter JW, Miller GA. Clinical evaluationof bacterial leakageof endodontic temporary filling materials. Journal of Endodontics 1996; 9: 459-62.
30. European Society of Endodontology (1994) Consensus report of the European Societyof Endodontologyon quality guidelines for endodontic treatment. International Endodontic Journal 1994;27:115-24.
31. Walton RE and Johnson WT, “Obturation,” in Principles and Practice of Endodontics, R. E. Walton and M. Torabinejad, Eds., 2002; 239–267,W. B. Saunders, Philadelphia, Pa, USA, 3rd edition.
32. Qualtrough AJE, Whitworth JM, and P. M. H. Dummer PMH. Preclinical endodontology: an international comparison. International Endodontic Journal 1999; 32(5): 406–414.
|