Introduction:
“Prevention is better than cure” the age old saying has been proven to be true in different situations time and again and is no different when applied to dental health. Reduction in oral diseases can be achieved through conducting appropriate oral health education programmes in the settings such as dental practice[1], schools[2], workplace[3], day-care and residential settings for older adults.[4] Focusing children on oral health practice activities at primary school age may have an important impact on their health-related behavior later in life as it is more feasible to modulate habits at young age, where as in adults established practices are difficult to modify[5].
Billions of children in the world of different age groups go to schools; these become the ideal locations for conducting educational programmes. 85% of the population in Himachal Pradesh resides in rural areas of which more than 35% constitute children[6]. This population is untouched by any preventive and educational dental health programmes, expressing poor knowledge about oral health practices and awareness. Literature reviews have also shown that numerous studies[7],[8],[9],[10] regarding oral health have been conducted and reported in India, but as far as Himachal Pradesh is concerned no data is available for the knowledge attitude and practices of the school children regarding oral health. The above factors prompted us to conduct the present study with the following objectives;. To assess the baseline Knowledge Attitude and Practices in oral health in school children in the age range of 7-14 in Sundernagar city, Himachal Pradesh. Changes observed in the Knowledge, Attitude and Practices in the same children following the oral heath education after 6 months
Materials & Methods
According to the Kaliyaperumal K. Guideline for Conducting Knowledge, Attitude and Practice (KAP) Study, the sample should be sufficiently large so as to represent the population yet not so large that the data collection and analysis is prohibitively difficult. At 95% confidence interval and 5% confidence level, the sample size calculated was 600. The epidimological study was carried out on 649 children in the age range of 7-14 years randomly selected from schools of Sundernagar city in Himachal Pradesh, India in 2012 to evaluate and compare the changes in their knowledge attitude and practice about oral health at baseline and six months after the implementation of organized preventive oral health education programmes in schools. Children younger than 7 years required indirect communication through the parents and children older than 14 years are usually not available for the subsequent visits because of their random shifting of institutions and hence they were not included in the study. Ethical approval to conduct the study was obtained from the Institutional Review Board of Himachal Dental College, Sundernagar. Written consent for the participation of the children in the study was obtained from the Principals of the concerned schools.
The inclusion criteria Schoolchildren (male and female) in the age range of 7-14, Children present on the day of examination Duration of Study. 6 months Number of investigators.[4] The children from each class were selected on the basis of systematic random sampling. Data on oral health KAP was collected by means of self administered close-ended questionnaires focusing on brushing frequencies, frequency of sugar intake, sugar and caries, role of fluoride, gum diseases, dental plaque and importance of deciduous teeth etc. The final questionnaire was subsequently discussed among the experts who judged the face and content validity of the question-naire. Reliability and internal consistency of the questionnaire was assessed using Cronbach’s coefficient of alpha test. Only questions scoring > 0.7 were approved for conducting the survey. A specially prepared computerized proforma in both English and Hindi was used which contained 17 questions,7 on knowledge (K), 5 on attitude (A) and 5 on practice (P). The questions were easily understandable by the children and did not contain high flown, technical or scientific words. The questionnaire was pretested by conducting pilot study among 10% of sample size to assess the children’s ability to understand the questions and answer them without any help. It took about 15 -20 min to fill all the questionnaires. Interpersonal communication was not allowed and the children were informed of the importance of answering the questions honestly. Questionnaires were completed under the supervision of investigators. The preventive programme to the children was delivered by giving oral health education lectures presented in power point in their local language Hindi. The technique of tooth brushing was demonstrated live to the children. The data obtained was recorded by using statistical package for social sciences version[11]. Associations were assessed using Chi square test and p value of less than 0.05 was considered significant.
Results
Knowledge and attitude regarding oral health at baseline and Changes Observed After 6 months of oral health education (Table1) 78.7% children considered brush to be the effective method of maintaining the oral hygiene. After the oral health education, the knowledge and attitude among children towards brushing being best method increased from 78.7% to 82% .Similarly at baseline evaluation 61% children had the knowledge that brushing should be done twice per day. Increase in thrice brushing and brushing after every meal group was noticed after 6 months.
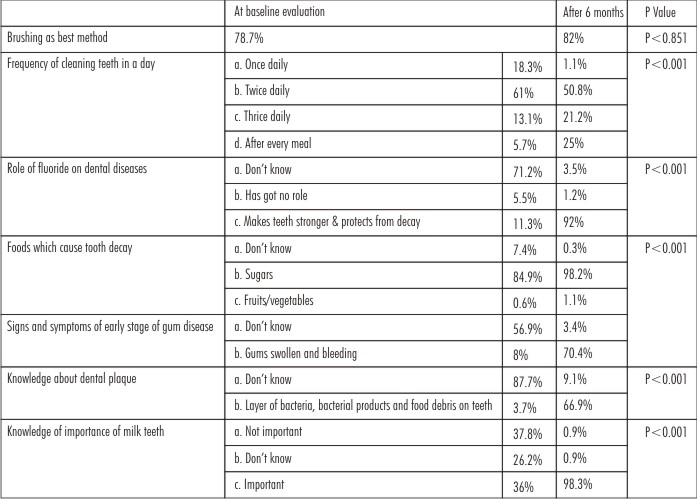 | Table 1:Knowledge And Attitude Of The Children At The Start Of The Study (Baseline) And Changes Observed Subsequent To Oral Health Education After 6 Months
 |
Knowledge and attitude towards Fluoride also statistically increased after six months as shown in Table 1. At base line most of the children were well aware with the fact that sugar is the main food which causes dental caries. The knowledge and attitude of the children regarding the role of sugar in dental caries further increased after oral health education. 56.9% and 87.7% children in the present study did not know about gum diseases and dental plaque respectively at the start of the study. After 6 months statistically significant improvement in their knowledge was seen. Most of the children in the present study had the knowledge that permanent teeth are important for various functions, but for deciduous teeth 37.8% children stated that they are not important and 26.2% children had no knowledge about the importance of milk teeth. Six months after the oral health education, 98.3% children were well aware with the importance of deciduous teeth. Oral Health Practices at baseline and Changes Observed After 6 months of oral health education (Table 2) At baseline 95.8% children were already using brushes to clean the teeth. 6 months after the oral health education, the number of children further increased to 99% .Only 39.1% were brushing twice a day initially, the frequency of brushing twice per day increased to 76.9% after six months. Of all the children, only 9.7% children were using fluoridated tooth paste to clean the teeth. After oral health education 93% children were aware that they were using Fluoridated toothpaste. At the start of the study 9.1% children knew about three sugar exposures and were consuming sugar thrice a day which then increased to 61.8% after 6 months. All the results were statistically significant.
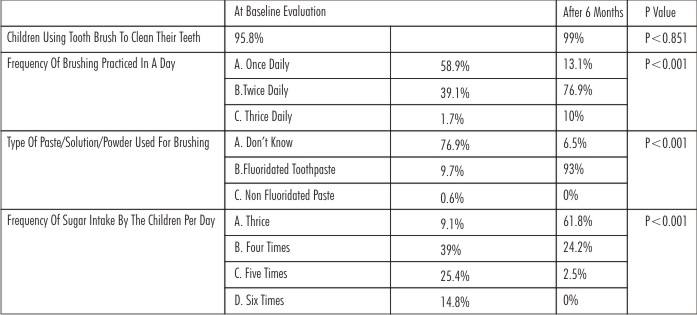 | Table 2:Oral Health Practices At The Start Of The Study (Baseline) And Changes Observed Subsequent To Oral Health Education After 6 Months
|
Discussion
The baseline evaluation of oral hygiene practice revealed that 95.8% children were already using brushes to clean their teeth (Table 2). The advertisements and some other educational programs on television have helped children to gain knowledge about the use of toothbrush. Similar results were seen with the study done by Humagain M[11] and Walsh M.M[12] in which 100% and 96% children respectively used tooth brush for cleaning the teeth. In the present study, though 95.8% children were using brushes to clean the teeth but only 78.7% children considered brush to be the effective method of maintaining the oral hygiene (Table 1).
The results were comparable with the questionnaire survey of Linn E L[13], where 99% children were using tooth brushes but 93% had the correct knowledge about tooth brush as the best effective tool for cleaning the teeth. When the children were educated about the importance of brushing in the present study, the knowledge among children about brushing being the best method increased from 78.7% to 82% (Table 1). These findings were comparable with the studies done by Chachra et al[10] and Shenoy RP[9] in which similar increase in the knowledge of brushing was observed after the oral health education At the start of the study, again 61% children (Table 1) had the knowledge that brushing should be done twice per day but regarding the practice, only 39.1% were brushing twice a day (Table 2). These results were comparable to Petersen PE[14], Harikiran AG[15] and Humagin M[11] in which at baseline 31.3%, 38.5% and 35.1% children were brushing twice. The children were educated to brush thrice or at least twice a day and statistically significant increase in the knowledge was observed. The frequency of brushing twice per day increased to 76.9% and thrice per day to 10%.(Table 2) More increase in twice brushing was observed than thrice brushing group, as most children could not brush their teeth in the afternoon in school.
The frequency of brushing also increased in the studies done by Walsh[12], Teng O[16], Peterson PE[14] and Shenoy RP[9] after the oral health education. 76.7% children at baseline had poor knowledge and attitude towards Fluoride (Table 1) and only 9.7% children were using fluoridated tooth paste to clean the teeth where as majority (76.9%) of children were not aware whether they were using fluoridated or nonflouridated toothpaste (Table2). These findings were similar to Harikiran AG[15] in which low values of knowledge attitude and practice towards the role of fluoride was noticed at the baseline. In contrast adequate baseline information was observed in the study done by Peterson PE[14] in which 74.9% children were aware of fluoridated tooth paste and were practicing with it. Jensen O[17], Smyth E[18] and Whye C[19] also showed the appreciable knowledge and attitude towards Fluoride tooth paste in the school going children. This lack of information in the present study was due to lack of proper guidance by the teachers or parents and due to lack of dental educational camps. After the implementation of oral health education in the school providing the information about the role of fluoride in the prevention of caries and strengthening of teeth along with the frequency of fluoridated toothpaste to be used, statistically significant (p<0.001). The results were similar in the study done by Shenoy RP[9] and Åstrøm AN[20] in which significant improvement in knowledge towards the sugar consumption was seen. It was observed that only 6 to 8% of the children at baseline knew correct answers about the signs and symptoms of gum diseases (Table 1).
Casual approach of the children and their parents towards the bleeding gums may be the basic cause for this neglect. Similar findings were observed in a study done in India by Punitha VC[21] and Shenoy RP[9] in which at baseline only 1.23% and 19% children respectively were aware of gum diseases, where as these findings were in contrast to studies done by Whye C[19] and Al-Omiri MK[22] in which 48.3% and 70% children respectively were aware that gingival bleeding reflects gingivitis. This might be explained by the fact that dental schools in the areas of above studies have been consciously promoting the role of prevention and proper management of young patient’s oral health. The children were educated about early stages of gingivitis in simple language as gum tissues swelling, redness and bleed on brushing in the present study and after six months the percentage of children having the correct knowledge increased from 8% to 70%. When the knowledge of the children about dental plaque was analysed at baseline, it was observed that 87.7% children in the present study did not know about dental plaque (Table 1). This lack of knowledge could reflect the dental health education, which was limited to certain levels of understanding and the contact with relevant dental personnel was confined only to the treatment hour. Poor knowledge about dental plaque among children was also noticed by Al Ansari J[23] and Whye C[19] where in both the studies found that 85.6% children were not aware of dental plaque. These findings were in contrast to the study done by Al .Omiri[22] and Humagain M[11] in which only 36.3% and 26.2% children respectively lacked knowledge about dental plaque. After the implementation of the programme in which correct knowledge about dental plaque was imparted 66.9% children had improved knowledge regarding dental plaque. Similar increase in the knowledge was observed in the study done by Hebbal M, Ankola AV, Vadavi D and Patel K[24] and D'Cruz A, Aradhya S[25] in which knowledge about plaque increased after oral health education. Most of the children in the present study had the knowledge that permanent teeth are important for various functions, but for deciduous teeth, 37.8% children stated that they are not important and 26.2% children had no knowledge about the importance of milk teeth (Table 2).
This lack of knowledge is due to the lack of information of the parents, teachers and caretakers. About 62% of the caretakers in the study done by Mani SA[26] agreed that it was not necessary to do fillings in deciduous teeth, with similar results reported from a study done by Szatko F[27] where two-thirds of the mothers agreed that care of deciduous dentition was unnecessary. Similar results were seen in the study done by Nagaveni[28] in which majority of parents of were unaware of the importance of the primary teeth. When the correct knowledge about the importance of milk teeth was imparted to the children in present study, the knowledge of children regarding the importance of deciduous teeth increased from 36% to 98.3% which was statistically significant. (p<0.001). (Table1).
Conclusion
Results of the study showed poor baseline knowledge, attitude and practices of the children towards oral health. When the oral health education was provided, increased Knowledge, attitude and practice towards oral health was observed. It can be concluded from the present study that the community based preventive programmes consisting of dental health education lectures are effective in changing the knowledge, attitude and practice about oral health of the children as well as in preventing and controlling the common dental diseases.
References
1. Baab, D. and Weinstein, P. Longitudinal evaluation of a self-inspection plaque index in periodontal recall patients. Journal of Clinical Periodontology.1986: 13: 313–318.
2. Stewart JE, Jacobs-Schoen M, Padilla MR, Maeder LA, Wolfe GR, Hartz GW. The effect of a cognitive behavioral intervention on oral hygiene. Journal of clinical periodontology. 1991;18(4):219-22.
3. Buischi, Y. A. P., Axelsson, P., Oliveira, L. B., Mayer, M. P. A. and Gjermo, P. Effect of two preventive programs on oral health knowledge and habits among Brazilian school children. Community Dentistry and Oral Epidemiology. 1994: 22: 41–46.
4. Schou L. Active involvement principle in dental health education. Community Dentistry and Oral Epidemiology 1985; 13: 128-32.
5. Kay, E. J. and Locker, D. Is dental health education effective? A systematic review of current evidence. Community Dentistry and Oral Epidemiology.1996: 24: 231–235
6. Age- group wise rural population and labour force-2011 census. Statistical outline of Himachal pradesh 2012-13; Department of economics & statistics Himachal pradesh, Shimla.
7. Shivaprakash PK, Elango I, Baweja DK, Noorani HH. The state of infant oral healthcare knowledge and awareness; Disparity among parents and healthcare professionals ; J Indian Soc Pedod Prev Dent 2009;27:39-43-8
8. Ajithkrishnan CG, Thanveer K, Sudheer H, Abhishek S. Impact of oral health education on oral health of 12 and 15 years old school children of Vadodara city, Gujarat state. Journal of International Oral Health. 2010;2:15–21.
9. Shenoy RP, Sequeira PS. Effectiveness of a school dental education program in improving oral health knowledge and oral hygiene practices and status of 12-to 13-year-old school children. Indian J Dent Res. 2010;21:253–9
10. Chachra S, Dhawan P, Kaur T, Sharma AK. The most effective and essential way of improving the oral health status education. J Indian Soc Pedod Prev Dent 2011;29: 216-21.
11. Humagain M. Evaluation of Knowledge, Attitude and Practice (KAP) About Oral Health Among Secondary Level Students of Rural Nepal - A Questionnaire Study WebmedCentral DENTISTRY 2011;2(3)
12. Walsh MM. Effects of school-based dental health education on knowledge, altitudes and behaviour of adolescents in San Francisco. Community Dent Oral Epidemiol 1985; 13: 143-7.
13. Linn EL. Teenagers' attitudes, knowledge, and behaviours related to oral health. J Am Dent Assoc. 1976:92:946-51
14. Petersen PE, Peng B, Tai B, Bian Z, Fan M. Effect of school-based oral health education programme in Wuhan City, Peoples Republic of China. Int Dent J. 2004;54:33–41.
15. Harikiran AG, Pallavi SK, Hariprakash S, Ashutosh, Nagesh KS. Oral health-related KAP among 11- to 12-year-old school children in a government-aided missionary school of Bangalore city; Indian J Dent Res 2008;19:236-42.
16. Teng O, Narksawat K, Podang J, Pacheun O. Oral health status among 12-year-old children in primary schools participating in an oral health preventive school program in phnom penh city, Cambodia, 2002. Southeast Asian J Trop Med Public Health. 2004 Jun; 35(2):458-62 .
17. Jensen O, Gabre P, Sköld UM, Birkhed D. Knowledge, attitudes and behaviour concerning fluoride toothpaste and toothbrushing in different age groups in Sweden. Community Dent Oral Epidemiol 2012; 40:175-184.
18. Smyth E, Caamaño F, Fernández-Riveiro P. Oral health knowledge, attitudes and practice in 12-year-old schoolchildren ; Med Oral Patol Oral Cir Bucal. 2007 Dec 1;12 (8):E614-20
19. Whye C, Lian, Tay SP, Chai SC, Cheong B, Shin et al. Oral health knowledge, attitude and practice among secondary school students in Kuching, Sarawak. Archives of Oralfacial Sciences(2010),5(1):9-16
20. Åstrøm AN, Mashoto KO. Changes in oral health related knowledge, attitudes and behaviours following school based oral health education and a traumatic restorative treatment in rural Tanzania. Norsk Epidemiologi 2012; 22 (1): 21-30
21. Punitha VC, Sivaprakasam P: Oral Hygiene Status Knowledge, Attitude and Practices of Oral Health among Rural Children of Kanchipuram District. Indian Journal of Multidisciplinary Dentistry 2011 Jan-feb;1(2):115-118.
22. Al-Omiri MK, Al-Wahadni AM, Saeed KN. Oral health attitudes, knowledge, and behavior among school children in North Jordan. J Dent Educ 2006;70(2):179-87.
23. Al-Ansari J, Honkala E, Honkala S. Oral health knowledge and behavior among male health sciences college students in Kuwait. BMC Oral Health 2003;3(1):1-6.
24. Hebbal M, Ankola AV, Vadavi D, Patel K. Evaluation of knowledge and plaque scores in school children before and after health education. Dent Res J. 2011;8:189–96.
25. D'Cruz A, Aradhya S. Impact of oral health education on oral hygiene knowledge, practices, plaque control and gingival health of 13- to 15-year-old school children in Bangalore city. Int J Dent Hyg 2013 May; 11(2):126-33.
26. Mani SA, Aziz AA, John J, Ismail NM. Knowledge, attitude and practice of oral health promoting factors among caretakers of children attending day-care centres in Kubang Kerian, Malaysia ; A preliminary study ; J Indian Soc Pedod Prev Dent 2010;28:78-83
27. Szatko F, Wierzbicka M, Dybizbanska E, Struzycka I, Iwanicka-Frankowska E. Oral health of Polish three-year-olds and mothers' oral health-related knowledge; Community Dent Health 2004; 21:175-80
28. Nagaveni N.B, Radhika N.B, Umashankar K.V. Knowledge, Attitude and Practices of Parents Regarding Primary Teeth Care of their Children in Davangere city, India. Pesq Bras Odontoped Clin Integr, João Pessoa 2011; 11(1):129-132.
|