Introduction
An accurate impression that provides the necessary marginal detail is not only required for good fit,but also for optimal esthetic results. Management of the gingival tissues while making an impression is one of the most challenging aspects of crown and bridge. This requires use of various tissue retraction techniques which is expensive, time consuming and unpleasant experience for the dentist.[1],[2] This can be avoided by using cordless impression methods where gingival retraction and an accurate void free impression can be made simultaneously. These impression techniques eliminate the use of retraction cords, cordless retraction materials or any other means of gingival tissue retraction.
Various cordless impression techniques for making impressions of subgingivally prepared margin have been described in literature. These methods make impregnated retraction cords unnecessary, and avoid their disadvantages. Leforgia A (1967)[3] studied the cordless tissue retraction for impressions in fixed prosthodontics and described various techniques for making cordless tissue impression like
1. relining preliminary impression
2. beading a cold cure acrylic resin tray
3. correcting an unacceptable final impression and
4. making an impression in an aluminium shell.
A new matrix impression system (Gus J. Livaditis 1998)[4],[5] was developed that incorporates the attributes of traditional methods and overcomes important deficiencies in registration of sub-gingival margins, gingival retraction and relapse, delivery of impression material subgingivally and simplification for making complex impressions.
M.R Dimashkieh et al (1995)[6] adopted a procedure for a void-free impression of tooth preparations for fixed prosthodontics known as prefabricated crown shell technique. A procedure was developed in which an impression was made in a preformed temporary crown shell for each tooth preparation. The result was an atraumatic and uncomplicated complete arch impression that incorporated an accurate impression of each prepared teeth.
In the present study two cordless impression techniques that is matrix impression system and prefabricated crown shell technique has been compared for dimensional accuracy.
Aim & Objective
The purpose of the present study is to compare dimensional accuracy of casts generated from two cordless elastomeric impression techniques and to give clinical recommendations and indications based on the study and observations.
Materials and Methods
Preparation of master model:
The master model (typhodont) consisting of articulated dentate maxillary and mandibular arches was used (Fig.1). Right mandibular first molar was removed to simulate a clinical case of three unit bridge. Mandibular second premolar and second molar were prepared as abutments with a finish line width of 1.2mm. Three sharply defined notches were placed on each prepared tooth as reference points. The reference points were referred as (Fig 2):
1. Point a - on buccal finish line of right mandibular 2nd molar.
2. Point b - centre of occlusal surface of right mandibular 2nd molar.
3. Point c - on lingual finish line of right mandibular 2nd molar.
4. Point d- on buccal finish line of right mandibular 2nd premolar.
5. Point e- centre of occlusal surface of right mandibular 2nd premolar.
6. Point f- on lingual finish line of right mandibular 2nd premolar.
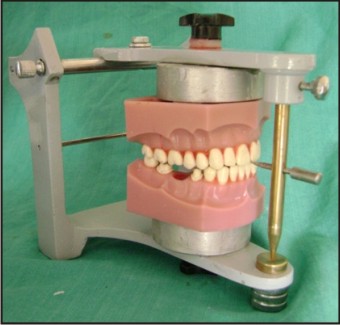 | Fig. 1 : Master Model
 |
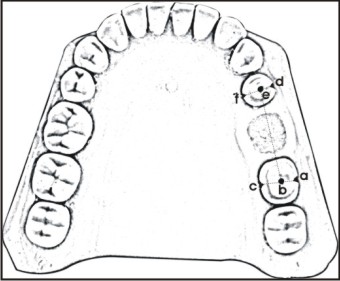 | Fig. 2 :Various Reference Points Made On Master Model
|
The various distances measured between reference points were:
Distances (a-b) and (d-e)which represented occluso-cervical dimension (vertical height) of right mandibular 2nd molar and right mandibular 2nd premolar respectively.
Distances (a-c) and (d-f)which represented bucco-lingual dimension (diameter) of right mandibular 2nd molar and right mandibular 2nd premolar respectively.
Distance (b-e)which represented inter-abutment distances between right mandibular 2nd molar and right mandibular 2nd premolar.
Addition silicones impressions (Aquasil, 3M ESPE, Germany) materials in various consistencies were used for making impressions. Tray used in the study was a rim lock perforated custom tray and prefabricated crown shells made of tooth colored acrylic (Fig.3).
 | Fig. 3 : Tray & Prefabricated Crown Used For Making Impressions.
|
Fifteen impressions were made for each group, casts were poured and categorized as:
Group A Matrix impression system[4] (Fig.4):
 | Fig. 4 : Matrix Impression Technique
|
A putty matrix was prepared over the selected abutments including one extra tooth adjacent to each abutment. The matrix was trimmed inter-dentally for escape of impression material and proximal surfaces of adjacent unprepared teeth were relieved to prevent wedging and distortion of matrix while seating. Heavy viscosity impression material was mixed, dispensed into the matrix and placed on the prepared abutments. Simultaneously a mix of medium body impression material was loaded in the stock tray and seated on the matrix to make a pick up impression. The impression was removed after complete polymerization of impression material.
Group B Prefabricated crown shell technique[6] (Fig.5):
 | Fig. 5 : Prefabricated Crown Shell Technique
|
Acrylic resin crowns were prepared on each prepared tooth with 0.75 mm thick base plate wax spacer adapted on each prepared tooth extending slightly apical to finish line of the preparation. A medium body elastomeric impression material was mixed and filled in preformed crown shell. The crown shells were seated over each tooth preparation to cover the finish line. Simultaneously a perforated metal stock tray was loaded with medium body elastomeric impression material and placed on the mandibular arch and a complete arch pickup impression was made.
Various measurements of master model and stone casts were done with the help of coordinate measurement machine (CMM, Llyod, Germany) with an accuracy of 0.0001 mm. All thirty casts were measured and the mean distances were taken as-
Vertical distances: a-b, d-e (molar height & premolar height respectively)
Horizontal distances: a-c, d-f, b-e (molar diameter, premolar diameter and interabutment distance respectively)
Observations & Results
After the readings were obtained they were compared with the dimensions on master model using one sample t-test and the comparisons in between the groups and within the groups were done by performing ANOVA. The difference between readings of stone casts and model was calculated as follows:
Mean difference = mean distance on master model – mean distance on stone model. The distances measured on the master model and casts obtained from two different groups were subjected to statistical analysis for comparisons. The observations and results of the study can be summarized in Table 1, Table 2, Table 3, Table 4 and Table 5.
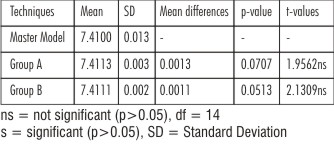
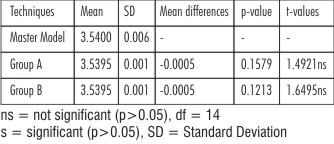 | Table 1: Basic statistics of molar height (a-b) measured on casts of different groups, compared with master model by one sample t-test.
|
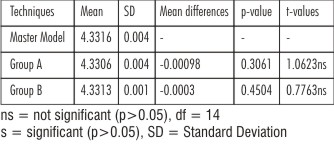 | Table 2: Basic statistics of premolar height (d-e) measured on casts of different groups, compared with master model by one sample t-test.
|
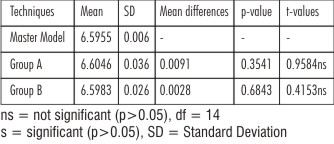
 | Table 3: Basic statistics of molar diameter (a-c) measured on casts of different groups, compared with master model by one sample t-test.
|
 | Table 4: Basic statistics of premolar diameter (d-f) measured on casts of different groups, compared with master model by one sample t-test.
|
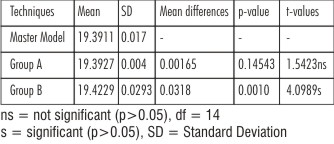 | Table 5: Basic statistics of inter-abutment distance (b-e) measured on casts of different groups, compared with master model by one sample t-test.
|
Discussion
All prosthetic rehabilitations are characterized by a sequence of well-structured clinical and laboratory steps, during which different kind of impressions are required. The success of the prostheses depends upon the accuracy and dimensional stability of the impression materials used and the impression techniques utilized. The exposure of the preparation margin in the gingival sulcus is a pre-requisite for a perfect impression and thereby improving the quality of indirectly fabricated restorations.
Deformation of gingival tissues during retraction andimpression procedures involves four forces: retraction,relapse, displacement and collapse. The aim ofgingival retraction is to atraumatically allow access for theimpression material beyond the abutment margin and tocreate space in order to provide sufficient thickness ofimpression material in gingival sulcus region so that it canbetter withstand the tearing forces encountered during removal of the impression[3],[7].
The purpose of the present study was to compare the dimensional accuracy of two cordless elastomeric impression procedures that is matrix impression system (Group A) and prefabricated crown shell technique (Group B). Among the various distances measured, the horizontal distances were measured to know the change in buccolingual dimensions and in interabutment distances, whereas vertical distances signified the occluso-cervical measurements.
It was observed from the study that none of the casts obtained from different techniques were similar to the master model in three dimensional measurements.
All impressions had a tendency to be slightly undersized in vertical dimensions (occluso-cervical) and oversized in horizontal dimensions (buccolingual and interabutment). This phenomenon occurred because of contraction of the impression material toward the tray walls, making the stone dies wider in horizontal aspect and shorter in vertical one[8].
The increase in horizontal distance seen may also be explained by linear setting expansion of the die material (Kalrock, 0.1% maximum) throughout the entire bulk of stone model. Also constraint is imposed by an effective adhesive on uniform shrinkage upon setting because of which abutments in resultant cast may tend to be greater distance apart than they are actually. This discrepancy in behavior may be attributed in part to the difference in the bond strength of tray adhesive. Marcinak (1980)[9] reported that the direction of dimensional change in impression material was dependent upon the bonding of the material to the tray. It was because of rigid tray and good adhesion to the tray, that the impression shrank toward the tray and produced a larger die.
In the present study from Table 1 and Table 2, it can be interpreted that the vertical distances that is molar and premolar height showed a decrease in dimensions as compared to the master model. The vertical dimension was less accurately reproduced by multiple mix impression than prefabricated crown shell technique but yet was not significant. This can be attributed to the fact that in prefabricated shell technique there is low polymerization shrinkage because of controlled bulk and uniform thickness of medium viscosity impression material in their respective crown shells. In matrix impression technique lesser accuracy may be because of greater polymerization shrinkage in low viscosity impression materials compared to medium viscosity impression material [10].
The Table 3 and 4 depicted that horizontal dimensions that is molar and premolar diameter showed an increase in dimensions as compared to master model. The horizontal dimensions were most accurately reproduced by Group B prefabricated crown shell technique as compared to Group A matrix impression system because putty is used as a matrix, which is somewhat resilient and hydraulic pressure creates undetectable distortion in the impression. Lesser accuracy of this technique can also be attributed to the fact that due to pressure of stock tray over the matrix, matrix can flex in bucco-lingual direction thus increasing the die in bucco-lingual dimensions[4].
The Table 5 showed an increase in interabutment distance as compared to the master model. The order of accuracy of various distances measured on the stone cast produced by different techniques deviated from the distances on master model was Group A > Group B. Prefabricated crown shell technique showed a statistically significant mean deviation. The results can be attributed to uneven or non-uniform bulk of impression material and variations in the direction of polymerization shrinkage as compared to matrix impression technique where bulk of material was controlled by fabrication of putty matrix which acted as a custom tray[4],[5].
On the basis of the study it was found that matrix impression technique showed more deviation as compared to prefabricated crown shell technique with respect to vertical distances and horizontal distances on the abutment teeth, but deviations were not statistically significant. Inter abutment distance showed statistically significant variation for prefabricated crown shell impression technique. So it can be stated that, each of these techniques is suitable for particular situation and advantageous in one or other way. For example multiple mix impression system uses a custom fabricated tray to control the bulk / thickness of elastomeric impression material and thus reducing the polymerization shrinkage. The matrix impression system used a precisely designed matrix which can provide a mean to better control the unpredictable dentogingival environment while making impressions, which significantly improves the gingival displacement and sulcular cleansing phases.
Pre fabricated crown shells were used to make void free, atraumatic and uncomplicated impressions for tooth preparations. This procedure used a prefabricated/custom made acrylic resin provisional crowns to make an intracrevicular impression for a complete crown preparation, which was followed by an pickup impression to make a working cast, this appoarch eliminated the need for displacement cord.
The present study showed a statistically significant distortion in prefabricated crown shell technique while recording inter abutment distance, so it is not recommended for a long span bridge framework. This technique is indicated while making impressions for fabrication of single crown. The limitation of the present study is that the dimensional changes in the present study were recorded indirectly by performing measurements on stone cast; the results include the variables of both impression and die materials. Also the results of this investigation might not be directly applied clinically because the oral environment was not simulated in this study.
Conclusion
Within the limitation of this in vitro study it can be concluded that all the impressions had a tendency to be oversized in horizontal dimensions and undersized in vertical dimensions. When comparing the accuracy of casts as per statistical analysis Group B (prefabricated crown shell technique) casts were less accurate in relation to inter abutment distance whereas all other distances produced statistically insignificant mean deviation from the master model.
It can be concluded that prefabricated crown shell technique is not recommended for a long span bridge framework but is well indicated while making cordless impressions for fabrication of single crown.
References
1. Effect of retraction materials on gingival health: A histopathological study. Phatale S, Marawar PP, Byakod G, Lagdive SB, Kalburge JV. J Indian Soc Periodontol. 2010 Jan;14(1):35-9.
2. A clinical study on the effects of cordless and conventional retraction techniques on the gingival and periodontal health. Al Hamad KQ, Azar WZ,Alwaeli HA, Said KN.J Clin Periodontol. 2008 Dec;35 (12):1053-8.
3. Cordless tissue retraction for impressions for fixed prosthesis.LaForgia A. J Prosthet Dent. 1967 Apr; 17(4):379-86.
4. Livaditis G J: The matrix impression system for fixed prosthodontics. J Prosthet Dent 1998 vol. 79, 208- 216.
5. Livaditis G J: Comparison of new matrix system with traditional fixed prosthodontic impression procedures. J Prosthet Dent 1998: 79(2): 200-207.
6. A procedure for making fixed prosthodontic impressions with the use of preformed crown shells.Dimashkieh MR, Morgano SM. J Prosthet Dent. 1995 Jan; 73(1):95-6.
7. Tissue displacement and impression techniques--part 1.Levartovsky S, Masri M, Alter E, Pilo R. Refuat Hapeh Vehashinayim. 2012 Jul;29(3):19-27, 55. Hebrew.
8. Nissan J, Laufer B,Brosh T , Assif D : Accuracy of three polyvinyl siloxanes impression techniques. J Prosthet Dent 2000:83:161.
9. Marcinak CF, Young A, Draughn RD, Flemming WR: Linear dimentional changes in elastic impression materials. J Dent Res 1980:59:1152-5.
10. Craig RG: Restorative dental materials ed. 10th st. Louis, CV M osby Co. 1985, pg.276.
|