INTRODUCTION
Loss of alveolar bone support is one of the characteristic signs of destructive periodontal disease and is generally considered to represent the anatomical sequela of the apical spread of periodontitis. The presence of periodontal osseous lesions is clinically significant in many ways. It relates to the associated loss of tooth support, to
the site specificity of periodontal destruction and to the possibility that ecological niches i.e. deep pockets and furcation involvement associated with some osseous lesions may represent site-specific risk factors or indicators for disease progression.1
Periodontal therapy involves two primary components. First is the elimination of the periodontal infection by eliminating the pathogenic periodontal microflora, which• induces substantial favorable clinical changes in the periodontium. However, the anatomic defect resulting from active periodontitis still persists and is represented clinically by loss of clinical attachment, increased probing depths, and radiographic bone loss. The substantial efforts made to alter this defect represent the second component of periodontal therapy. Regenerative treatment has as its goal elimination of periodontal defects by regenerating the lost periodontium including bone, cementum and periodontal
ligament.2
At present, bone grafting is the only modality of therapy for which there is histologic evidence, in humans, of regeneration of new attachment composed of new bone, new a cementum and new periodontal ligament coronal to the base of a
osseous defect.3 Recently one new bone graft material ossifi (equinox medical technologies, Holland) is introduced. It is a synthesized combination of hydroxyapatite and â- tricalcium phosphate in a 70/30 ratio, creating a new molecule with new characteristics. It has 90% interconnected porosity. When it is placed in bone defect, it occupies 10% of the defect space leaving 90% of the space for regeneration of bone. It has been developed in such a way that it mirrors the chemical composition and structure of human bone. The biologic similarity to natural bone results in optimal biocompatibility and ensures that this material is well tolerated by the body. The purity and synthetic nature of this
material ensure safe grafting without the risk of transmitting viral infections..
CASE REPORT
We are presenting a case report of 2 patients which reported to department of Conservative Dentistry, Himachal Institute of Dental Scienes, Paonta Sahib,.One was 48 years old male with chief complaint of food lodgement and second
was 35 years old male with chief complaint of bleeding gums and sensitivity. Medical history was
negative for any other coexisting disease. We are presenting a case report of 2 patients which reported to department of Conservative Dentistry, Himachal Institute of Dental Scienes, Paonta Sahib,.One was 48 years old male with chief complaint of food lodgement and second was 35 years old male with chief complaint of bleeding gums and sensitivity. Medical history was negative for any other coexisting disease.
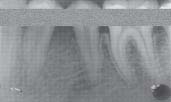
Clinical examination revealed generalized 6-7 mm pockets with bleeding on probing. Halitosis and pus exudation was also present. Radiographic evaluation consisted of orthopantograph and intraoral periapical radiographs using illimeter grid with vertical bone defect in 36 (case 1) and 46 (case 2).
[Image 1]
 | case 2
 |
Laboratory investigations included Hemoglobin level, Total Leukocyte Count, Differential Leukocyte Count, Bleeding Time, Clotting Time and Random Blood Sugar. Based on clinical and radiological examination a diagnosis of chronic generalized periodontitis was made.
 | case 1
|
 | case 2
|
OSSIFI PLACED IN DEFECT
 | case 1
|
 | case 2
|
 | case 1
|
 | case 2
|
SURGICAL PROCEDURE
The surgical procedure was performed utilizing local anesthesia, 2% xylocaine with epinephrine 1:100,000. Intra sulcular incisions with reflection of full thickness flaps were utilized to retain as much soft tissue as possible in order to obtain primary closure. Debridement and root planing were accomplished with hand instruments (Gracey Curettes). After cleaning, the surgical area was irrigated with sterile saline. The surgical area was carefully inspected to ensure that
the debridement procedure has been completed satisfactorily. Biphasic calcium phosphate (ossiffl® was
emptied into a sterile dappen dish and prepared by adding 4 to 6 drops of saline until the mixture was paste like in consistency. It instantly gels to a cohesive mass. In the periodontal osseous defects small increments of graft material were added, starting from the bottom of the defect and adapted well to its configuration. The granules were lightly packed
without overfilling of the defect space. Every effort was made to avoid contamination of the debrided root surface with saliva and blood until the graft material had been applied. The soft tissue flap was then repositioned at the original level and closed with interrupted direct loop sutures using 3-0 Mersilk sutures .Care was taken to achieve a tension free primary closure of flap on suturing. Surgical site was protected by applying a periodontal dressing.
POST-OPERATIVE CARE
1. The patients were advised to rinse with 0.2% chlorhexidine gluconate solution twice daily for 14 days for assistance in plaque control.
2. The patients were advised to avoid chewing in the surgical area for the same period of time.
3. The patients were informed not to brush at the surgical site or manipulate it in any way for 10 days. They were prescribed medications which included a non steroidal anti-inflammatory agent Ibuprofen 400mg thrice a day for post operative discomfort and Doxycycline hydrate 100 mg at a dose of 200 mg the day of surgery and 100 mg per day
for the next 6 days to prevent infection.
After 7 to 10 days dressing, sutures and any plaque present in the area was removed. The recall appointments were scheduled at 3 months and 6 months post surgically fir soft tissue evaluation, plaque control, and radiographic evaluation.
DISCUSSION
Biphasic calcium phosphate (ossifi)® is a synthetic graft material. Being alloplastic in nature it does not increase the patient morbidity and does not require second surgical site as in case of autografts. It is a synthesized combination of
hydroxyapatite and 13-tricalcium phosphate in a 70/30 ratio and has calcium phosphate in its purest form. It has a bioceramic matrix that is extremely biocompatible and highly osteoconductive. It mirrors the chemical composition and structure of human bone and is well tolerated by the body. When it is placed in a bone defect, it only occupies
1 of the defect space leaving 90%of the space for regeneration of new bone. The pore size of this material is highly reproducible and constant. This reproducible interconnected porosity combined with a large granular inner surface area provides the highest degree of osteoconductivity through clot stabilization, vascularisation, cell adhesion and penetration of host bone repair into the inner part of the graft material. Biphasic calcium phosphate (ossifif enhances the biological
resorption of the granule and ensures optimum bone ingrowth and formation.
The mean percentage of defect resolution at 3 months and 6 months in test sites was 53.65% and 67%.
Biphasic calcium phosphate (ossifi)® improves the healing outcomes regarding probing depth reduction, osseous defect resolution and gain in clinical attachment. Better biocompatibility, excellent handling properties and improved tissue response to the material are the definite benefits of using biphasic calcium phosphate (ossifi)® enhances the biological resorption of the granule and ensures optimum bone in growth and formation
REFERENCES
1. Papapanou PM, Tonnetti MS. Diagnosis and epidemiology of periodontal osseous lesions. Periodontol 2000; 2000; 22:8- 22.
2. Garrett S. Periodontal regeneration around natural teeth. Ann Periodontol 1997; 7: 621-666.
3. Yukna RA. Synthetic grafts and Regeneration. In: Periodontal Regeneration Current Status and Directions. PoIson AM,
Quintessence Publishing Co. Inc. 1994:103-112.
4. Addy M. The use of antiseptics in periodontal therapy. In: Lindhe J, Karring T, Lang NP, Clinical Periodontology and Implant Dentistry. Blackwell munksgaard, 4th edition. 2003; 464-493.
5. Klokkevoid PR et al. General principles of periodontal surgery. In: Carranza FA, Newman MG. Takel HH. Clinical Periodontology. Saunders 9th Edition 2003; 804.
6. Kornman KS, Robertson PB. Fundamental principles affecting the outcomes of therapy for osseous lesions. Periodontol 2000; 2000: 22:22-43.
7. Nery EB, Legeros RZ, Lynch KI et al. Tissue response to biphasic calcium phosphate ceramic with different ratios of
HA/I3TCP in periodontal osseous defects. J Periodontol 1992; 63: 729-735.
8. Newman MG et al. Effect of 0.12% chlorhexidine on bacterial recolonization after periodontal surgery. J Periodontol 1989; 60: 577-89.
9. Simon RM, Charles MC, John WR et al. In vivo comparison of synthetic osseous graft materials: A preliminary study. 3
Clin Periodontol 1999; 26(4): 239-245. |