Introduction
Supernumerary teeth are those that are in excess of normal complement and mimic the normal shape.[1] The prevalence of the supernumerary premolars in permanent dentition is between 0.075-0.26%.[2],[3] Supernumerary teeth can occur as single, multiples, unilaterally or bilaterally and in the maxilla, the mandible or both. Cases involving one or two supernumerary teeth most commonly affect the anterior maxilla, followed by the mandibular premolar region.[4] The etiology and mechanisms that can give rise to supernumerary teeth in the maxillary midline or premolars are fairly similar. Gardiner suggested three possible mechanisms, including an abnormal proliferation of the dental lamina, an additional follicle, and an extension of the dental lamina after the deciduous as well as permanent follicles (post-permanent type). [5]
We report here, two cases with supernumerary non-syndromic premolars.
Case 1
A 13 year old boy presented with the chief complaint of pain on both the sides of the jaw in the front of ear and restricted mouth opening since 2 weeks. History revealed that patient met with a road traffic accident 4 years back and was treated for the same.
Extraorally, patient had bilaterally symmetrical face, non tender and no clicking on palpation in the TMJ region. The patient could open the mouth to maximum with difficulty because of pain. Intraoral examination revealed permanent dentition Angles Class1 molar relationship with well aligned maxillary and mandibular arch with fair oral hygiene. No other significant abnormalities were seen during examination.
Patient was then advised for OPG (Fig.1) Radiograph did not reveal any significant findings in relation to TMJ. Surprisingly, two separate well developing supernumerary premolars were observed and another questionable sac like structure observed near the apical region of distal root of 46. (Fig 2).
 | Fig 1 : Opg Showing The Presence Of Supernumerary Mandibular Premolars On Right Side
 |
 | Fig 2 : Iopa Radiograph Showing Supernumerary Mandibular Premolars In Various Stages Of Development
|
Case 2
A 15 year old boy patient reported for the treatment of malocclusion. On clinical examination, 16 and 26 were carious. An interesting finding of bilateral maxillary erupted supernumerary premolars was noticed (Fig 3) causing crowding in that area. Supplemental premolars were morphologically similar to the first premolars. OPG did not reveal any other developing, unerupted supernumerary teeth in relation to premolars.
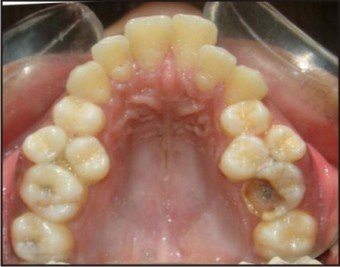 | Fig 3 : Showing Supplemental Maxillary 1st Premolars On Right And Left Side
|
In both the above cases, history from the child and the parents did not help in any hereditary aetiology.
Treatment and follow up
In first case pain got relieved after taking anti-inflammatory drug for 3 days. Since the erupted molars and premolars were asymptomatic and vestibular tenderness was absent, developing supernumerary premolars were kept under observation. In second case patient is undergoing orthodontic treatment after bilateral extraction of supplemental maxillary first premolars.
Discussion
Multiple supernumerary teeth are frequently recognized as a part of characteristics of cleidocranial dysplasia and Gardner syndrome.[6],[7] However, it is rare to find multiple supernumeraries in individuals with no other associated disease or syndrome. The most frequent supernumerary teeth identified are mesiodentes, followed by premolars and fourth molars or distal molars.[8],[9] Yusof [10] reviewed most of the literature and found that a predominance of non-syndrome multiple supernumerary teeth occurred in the mandibular premolar area. Solares and Romero,[11] in their comprehensive review of supernumerary premolars, found male to female ratio of 3 to 1, mean age of 16.4 years, and an extremely high occurrence rate of 74% for mandibular premolars. Unlike other supernumeraries, they are more likely to develop in mandible than maxilla and usually resemble normal premolars in shape and size (Stafne, 1932). Stafne also states that there is a tendency for supernumerary teeth to commence their development later than the normal for teeth of that region.[12]
Complications associated with the presence of supernumerary teeth include enlarged follicular sacs, cystic degeneration, nasal eruption, malposition of adjacent teeth, over retention of primary teeth, delayed eruption of permanent teeth, loss of space, impaction, diastema, loss of vitality, and root resorption.[13],[4]
The timing for surgical removal of supernumerary premolars is still controversial. Hanratty[14] suggested removal of more developed supernumerary premolars be accomplished soon after diagnosis, but less developed premolars be left in situ and removed later in order to avoid damage to adjacent structures and allow for bone regeneration. However, asymptomatic supernumerary teeth may be left in place and immediate removal indicated only if any of the aforementioned complications are evident.[15]
Also if a supplemental tooth is present and erupted, it may be difficult to determine which is the supplemental and which is the tooth of the normal dental series. In these circumstances, assuming both teeth are healthy, it is logical to extract the tooth most displaced from the line of the arch for the relief of crowding.[4]
A relatively high percentage of cases with supernumerary teeth are accidentally found during radiographic examinations. A special phenomenon of supernumerary premolars reported in the literature is their recurrence and new development of supernumerary teeth.[16],[17],[18] Anegundi et al reported a unique case of multiple premolars in all four quadrants that were distributed unevenly. A series of radiographs taken over four years demonstrated further sequential developing bilateral supplemental premolars in the maxilla, where they are considered rarest.[19] Supernumerary premolars commonly occur in several regions of the same mouth, so the finding of one indicates radiographic examination of the other premolar regions. It has been reported that up to 24% of patients with an anterior maxillary supernumerary may later develop supplemental premolars.[4]
The dental lamina is not completely resorbed and is reactivated at the time of crown completion of the normal permanent teeth, which can create multiple supernumerary teeth especially in the premolar region.[13] Lin[13] et al reported a case with overall nine supernumerary teeth which were found in the following 2 years. So it is sometimes difficult for clinicians to make a proper treatment plan for cases with multiple supernumerary teeth because of their recurrence or newly developed supernumerary teeth, especially in the premolar region. Thus multiple phases of treatment may be necessary in order to achieve an ideal clinical result. Each case must therefore be considered individually concerning its treatment. Close observation with regular radiographic control is recommended. Thus patient follow up is essential.
References
1. Bhaskar SN. Synopsis of Oral Pathology. St Louis: C V Mosby 1961. p. 17
2. Hyun HK, Lee SJ, Ahn BD, Lee ZH, Heo MS, Seo BM, et al. Nonsyndromic multiple mandibular supernumerary premolars. J Oral Maxillofac Surg 2008;66:1366–9.
3. Kaya GS, Yapici G, Omezli MM, Dayi E. Non-syndromic supernumerary premolars. Med Oral Patol Oral Cir Bucal Epub 2010 June 1
4. Shah A, Gill DS, Tredwin C and Naini FB. Diagnosis and Management of Supernumerary Teeth. Dent Update 2008; 35: 510-520
5. Gardiner JH. Supernumerary teeth. Dent Pract 1961;12:63-73
6. Ida M, Nakamura T, Utsunomiya J. Osteomatous changes and tooth abnormalities found in the jaw of patients with adenomatosis coli. Oral Surg 1981;52:2−11.
7. Jansen BL, Kreiborg S. Development of the dentition in cleidocranial dysplasia. J Oral Pathol Med 1990;19:89−93.
8. Montenegro PF, Castellon EV, Aytes LB, Escoda CG. Retrospective study of 145 supernumerary teeth. Med Oral Patol Oral Cir Bucal 2006;11:E339−44.
9. Umweni AA, Osunbor GE. Non-syndrome multiple supernumerary teeth in Nigerians. Odontostomatol Trop 2002;25:43−8.
10. Yusof WZ. Non-syndrome multiple supernumerary teeth: literature review. J Can Dent Assoc. 1990;56:147–9.
11. Solares R, Romero MI. Supernumerary premolars: a literature review. Pediatr Dent 2004;26:450−8.
12. Supernumerary Premolar Teeth in Siblings. Scanlan PJ, Hodges SJ. BJO1997; 24(4): 297-300
13. Lin YT, Chang SW, Lin YTJ. Delayed formation of multiple supernumerary teeth. J Dent Sci 2009;4(3):159−164
14. Hanratty WJ. Odontectomy of seven impacted supernumerary bicuspids. J Am Dent Assoc 1960;61:80−2.
15. Sharma U, Gill NC. Multiple Non-Syndromic Supplemental Premolars- A Case Report. IJCD 2010;1(3):29-31
16. Poyton GH, Morgan GA, Crouch SA. Recurring supernumerary mandibular premolars: report of a case of postmature deve lopment. Oral Surg Oral Med Oral Pathol 1960;13: 964−6.
17. Stevenson W, McKechnie AD. Recurring supernumerary teeth: report of a case. Oral Surg Oral Med Oral Pathol 1975;40:76−80.
18. Shapira Y, Haskell BS. Late developing supernumerary premolar. J Clin Orthod 1981;15:571.
19. Anegundi RT, Tavargeri A, Indushekar KR, Sudha P. Sequential development of multiple supplemental premolars four year follow up report. NYSDJ 2008;74(1):46-49.
|