|
|
|
| Unilateral Maxillary Sinusitis Of Dental Origin - A Case Report. |
Vandana Bhardwaj 1
1 Assistant Professor, Dept. Of Conservative - P.G.I.D.S, Rohtak
|
| Address For Correspondence |
Dr. Vandana Bhardwaj
Assistant Professor, Dept. Of Conservative
P.G.I.D.S, Rohtak
Haryana, India.
Pincode 124001
Email id : doc.vanbhardwaj@gmail.com |
| Abstract |
| Knowledge of the anatomical relationship between the maxillary sinus floor and the maxillary posterior teeth root tips is important for the preoperative treatment planning of maxillary posterior teeth. In view of the proximity of the maxillary sinus floor and maxillary root tips, clinicians must be particularly cautious when performing dental procedures involving the maxillary posterior teeth. Maxillary sinusitis (inflammation of maxillary sinus) may be of dental origin. The dental causes of maxillary sinusitis include peri-apical infection, perio -dontal disease or perforation of the antral floor and antral mucosa at the time of dental extraction. Roots and foreign objects forced into the maxillary sinus at the time of operation may also be the causative factors of sinusitis. Present article highlights a case of accidental extrusion of sodium hypochlorite into maxillary sinus and its successful management. |
|
| Keywords |
| odontogenic sinusitis, sodium hypochlorite, sinus, extrusion |
|
| Full Text |
Key message: The result of accidental sodium hypochlorite extrusion is unpredictable with no set level in terms of concentration and volume that determine the severity of patient symptoms. The early recognition and appropriate management of these complications by the dental practitioner is essential in case an extrusion occurs to ensure best clinical practice.
Introduction
Endodontic implications of the maxillary sinus include extension of periapical infections into the sinus, the introduction of endodontic instruments and materials beyond the apices of teeth in close proximity to the sinus.[1] Three cases of inadvertent injection of sodium hypochlorite into the maxillary sinus have been reported.[2],[3],[4]
Odontogenic sinusitis accounts for approximately 10% of maxillary sinusitis cases[5]. However, more recent works have shown that it is not a rare condition [6]. The alveolar bone can become thinner with increasing age,particularly in areas ,so that root tips may protrude into the sinus cavity and occasionally the expansion can be so extreme so as to leave only the sinus mucoperiosteum.[7]
Case Report
A 20 year old female was allotted to senior student of fifth year to treat upper right second premolar. It was determined that a senior student (fifth-year student) administered the local anesthetic. The pulp was extirpated and cleaning and shaping was completed with 2.5 % sodium hypochlorite solution and saline. Patient complained of discomfort on irrigation which was overlooked by student.
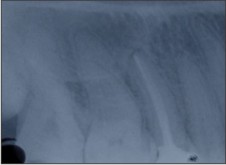
One day later, patient reported back with complaint of watery substance draining from her right nostril. The drainage continued several times that evening and increased on bending. She had continuous severe pain that traveled from jaw up to temple. Difficulty in breathing and pressure in the right side of the cheek were also reported by the patient. Diagnostic radiograph (Fig-1) showed roots of second premolar in very close proximity with floor of maxillary sinus which was unseen by senior student. Occipitomental radiograph (Fig-2) shows the radiopacity in the involved sinus and radiolucency in the normal sinus. The radiopacity in the affected right maxillary sinus is caused by the presence of fluid in the sinus.
 | Fig-1 Diagnostic Radiograph Showed Roots Of Second Premolar In Very Close Proximity With Floor Of Maxillary Sinus Which Was Unseen By Senior Student.
 |
 | Fig-2 Occipitomental Radiograph Shows Radiopacity In The Involved Sinus And Radiolucency In The Normal Sinus.
|
Immediately sodium hypochlorite accident was suspected. After removing the temporary dressing, a profuse hemorrhage was discharged from the root canal. Patient described her specific intolerable discomfort on irrigation. Under rubber dam isolation, copiously irrigation with saline was done cautiously without inducing apical pressure. The correct working length was determined and root canal was prepared biomechanically using hand instruments. The canals were closed with cavit and patient was contacted everyday to monitor recovery.
Antibiotic was prescribed against secondary infection and analgesics, Nasal decongestant and antiallergic were also prescribed. Steam inhalation was also advised. Medications are described in (Table - 1).
 | Table - 1
|
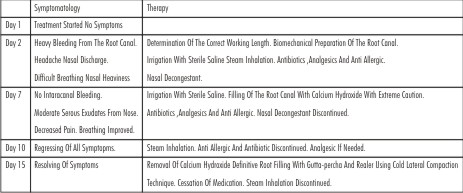
The symptomatology and therapy of the case in following days is summarized in (Table-2). On day 15 the root canal was dry when the calcium hydroxide dressing was removed. Tooth was obturated with gutta-percha and root canal sealer using lateral condensation. (Fig-3).
 | Table - 2
|
 | Fig-3 Tooth Was Obturated With Gutta-percha And Root Canal Sealer Using Lateral Condensation
|
Discussion
A good quality periapical radiographs are essential for preoperative diagnosis of teeth scheduled to undergo treatment. However, this radiography is limited by the fact that information is rendered in only two dimensions. Interpretation is more difficult when the background pattern is complex[8]. This often occurs in the posterior maxillary region, where roots of teeth overlap and anatomic structures such as the maxillary sinus and the zygomatic buttress are present.[9] In the present case such a proximity of root apices with sinus can be seen on the periapical radiograph (Fig. 1) which was unseen by senior student. As a consequence, instrumentation beyond the apical foramen resulted in communication between the palatal canal and sinus.
Additionally, extreme pressure during irrigation and binding of the irrigation needle tip in the root canal with no release for the irrigant to leave the root canal coronally resulted in this situation. Profuse haemorrage and pain particularly during irrigation particularly in palatal canal depicted close relation of sinus with palatal root.
It was concluded by Frank that the effects of the irrigant on the patient depend on the type, concentration and amount of exposure with the tissue to the used solution. The use of a 2.5% concentration of the irrigant must have been helpful for the relatively milder symptoms in the present case.The expected sequel of parathesia, intraoral or extraoral swelling, intersititially bleeding leading to echymosis were not experienced.
As cases described by Ehrich et al and Zairi et al recovered probably because of immediate drainage.[3],[4] Unfortunately, immediate drainage was not possible in present case. Eventually, unilateral maxillary sinusitis manifested. Lack of drainage in case reported by Kavanagh and Taylor necessitate the surgical drainage under general anaesthesia.[2] Three months later, tooth was extracted because of continued localized pain. Fortunately, symptoms were controlled early and no serious complications developed in present case. Thereby, giving us chance to treat patient with non surgical root canal treatment.
In addition ,no specific treatment can reverse the damages caused due to sodium hypochlorite .Mainstay of treatment is supportive including control of discharge, pain relief and prevention of secondary infection. Antibiotic therapy is highly recommended to prevent the risk of developing secondary infection.
To decrease oedema around the ostia so as to facilitate drainage and allow sinus oxygenation.[10] Topical decongestants drops or sprays are advocated and are beneficial, provided that their use is not extended beyond 3–5 days as a result of significant rebound effect.[10]
The etiology of such emergency is non evaluation of radiograph, incorrect determination of endodontic working length, iatrogenic widening of the apical foramen, or wedging of the irrigating needle. Clearly, precautions must be undertaken to prevent such mishaps. The irrigating needle has to be fixed to the syringe and must not be wedged into the root canal. During irrigation a low and constant pressure should be used and the operator must ensure that excess irrigant leaves the root canal coronally via the access cavity. However, it has been shown that contact between the periapical tissues and the irrigant cannot be avoided completely. Therefore, a dilute concentration of the irrigant that still retains adequate disinfective properties is recommended.
References
1. Hauman CHJ, Chandler NP, Tong DC.Endodonticimplications of the maxillary sinus: a review.International Endodontic Journal 35, 127–141, 2002.
2. Kavanagh CP, Taylor J. Inadvertent injection of sodium hypochlorite into the maxillary sinus. Br Dent J1998;185;336-337.
3. Ehrich DG, Brian JD Jr, Walker WA. Sodium hypochlorite accident: inadvertent injection into the maxillary sinus. JEndod 1993;19:180-182.
4. Zairi A, Lambrianidis T (2008). Accidental extrusion of sodium hypochlorite into the maxillary sinus. Quintessence Int. 39:745-748
5. Mehra P, Murad H. Maxillary sinus disease of odontogenic origin. Otolaryngol ClinNorth Am 2004;37:347–64
6. Obayashi N, Ariji Y, Goto M, et al. Spread of odontogenic infection originating in the maxillary teeth: computerized tomographic assessment. Oral Surg Oral Med OralPathol Oral Radiol Endod 2004;98:223–31.
7. Brook I. Sinusitis of odontogenic origin. Otolaryngol Head Neck Surg 2006;135:349–55
8. Kundel HL, Revesz G. Lesion conspicuity, structured noise, and film reader error.Am J Roentgenol 1976;126:1233–38.
9. Orstavik D. Radiology of apical periodontitis. Essential endodontology: preventionand treatment of apical periodontitis, ed 1. Oxford, UK: Blackwell Publishing Ltd;1998:131–52.
10. Pinheiro AD, Facer GW, Kern EB (1998) Sinusitis: Current concepts and management. In: Bailey, BJ, ed. Head and NeckSurgery – Otolaryngology, 2nd edn. Philadelphia, USA: Lippincott-Raven Publishers, 441–55.
|
|
|
|
|
|
|