Introduction
Fusion, Gemination and Dens-in dente are the developmental abnormalities of the shape of teeth commonly seen in anterior teeth. The gemination occurs when two teeth develop from one tooth bud as a result of which the patient has a larger tooth but total number of teeth is normal. In contrast the patient with fusion appears to have a missing tooth. Fusion of teeth occurs by union of two tooth germs which are normally separated and it may be either complete or incomplete depending upon the stage of development of the teeth when the union occurs.[1] The incidence of fusion is 0.5% and there is no predilection of sex.[2] Occasionally two independent root canals which may originate from same or different pulp chambers are seen. In geminated tooth, division is usually incomplete and results in a large tooth crown that has a single root and a single canal.[1] In gemination, the normal complement of teeth is seen in the arch whereas in fusion there is one tooth less than the normal complement. Confusion arises when fusion occurs with a supernumerary tooth as the number of teeth in the arch remains normal.[2] The term ‘double tooth’ has been suggested to cover both of these possibilities when the true etiology cannot be determined.[3]
Dens invaginatus is a developmental variation that mostly involves the permanent maxillary incisors and is thought to be due to infolding in the crown of the tooth before calcification. It frequently occurs bilaterally so if one tooth is affected, its homologous should also be investigated. It is detected mostly by chance on radiography. The invagination in the surface of the tooth acts as a pathway that allows entry of irritants into an area which is separated from pulp by a thin layer of enamel and dentin and is more prone to development of caries.[1] This invagination is frequently limited to the crown of the tooth with normal morphology of the root and root canal whereas in most severe cases, the invagination can reach upto the apical portion of the root.[4]
A tooth with an acute periradicular abscess is very painful to biting pressure, percussion, and palpation. Pulp vitality tests are negative and tooth exhibit varying degrees of mobility and the radiograph may show anything ranging from a widened periodontal ligament space to periradicular radiolucency.[5]
The following case report describes the endodontic management of a maxillary right central incisor that could be diagnosed as fusion, gemination or dens invaginatus.
Case Report
A 23-year-old male reported with the chief complaint of pain in the maxillary incisor region. Elaborating the history of present illness pain was continuous in nature and radiated to right side of the face. Pain subsides on taking medication.The tooth was symptomatic and tender to percussion. The labial cortical plate was tender on palpation. Electric pulp tester and thermal tests had no response from the tooth. There was no swelling, fistula or any sinus formation.Clinical examination also revealed themaxillary right central incisor had an anomalous clinical crown. The tooth was wider bucco-palataly but it had the same dimensions mesio-distally in comparison to the contralateral one. (Figure 1 & 2) The tooth was carious in the middle portion of the cingulum region. Probing revealed no periodontal pockets around the tooth. Intraoral periapical radiograph showed that tooth had two separate root canals- one upto full length and one smaller. (Figure 3) Radiolucency was associated with the tooth and itwas diagnosed as periapical abscess with a necrotic pulp.CT scan of the region showed two different root canals in central incisor and tooth was widened labio-palatally (Figure 4).
 | Figure 1. Shows Carious Right Maxillary Central Incisor Widened Labio-palatally
 |
 | Figure 2. Shows Maxillary Cast With Widened 11 Labio-palatally
|
 | Figure 3. Shows Periapical Radiolucency W.R.T 11
|
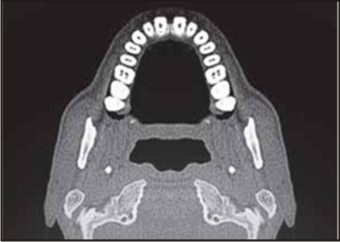 | Figure 4. Ct Scan Of The Maxillary Region Showing Two Root Canals.
|
The access was made through the centre of the cingulum of the tooth without anaesthesia using the round carbide bur. The pus was released as soon as pulp chamber was reached, Two separate root canal orifices were found on the same level of the pulp chamber floor. Canal orifices were in bucco-palataly order. Gentle filing was done to drain the pus. Copious irrigation was done using the 5% sodium hypochlorite. After the pus was drained, working length was measured using the radiographic method.
Biomechanical Preparation was done using the Ni-Ti Files using the step-back technique. Irrigation was done with Sodium hypochlorite and canals were dried using the paper-ponts and alcium-hydroxide dressing was given and access was sealed with Orafil (temporary filling material).Patient was prescribed broad spectrum antibiotics and analgesics for 5 days.
After a week there were no signs of pus discharge, tooth was non-tender and canals were dry, the tooth was obturated by cold lateral condensation of gutta-percha with endofill as sealer (Figure 5) and composite restoration was done.
 | Figure 5. Obturated Tooth With Two Root Canals
|
Discussion
Dental anomalies are seen in both the primary as well as the permanent dentition.[6] Gemination and fusion are encountered most often in the anterior teeth region of the primary and permanent dentition with a greater frequency in permanent dentition.[7] The malformations or any abnormality in tooth is often a challenge to the dentist in respect to its specific diagnosis of developmental disturbance as well as in planning the treatment to restore its form and function.[8] Gemination and fusion have overlapping clinical and radiographic appearance with each other. Fusion and gemination may be differentiated from each other by the presence of two entirely separate roots or one single root and by counting the number of teeth in the arch.[6] In the present case the number of teeth was normal and no differentiation could be made between fusion and gemination. However, it may mesiodens which is fused with maxillary central incisor palatally causing the buccal displacement of the tooth as well.
Before endodontic therapy, the dentist must be prepared for any deviations in root canal anatomy and should give some time to careful preoperative radiographic evaluation, that may enable him to identify any such abnormalities thus increasing the prognosis of the treatment and restoring the form and function of the tooth.
In the present case, the nature of the abnormality i.e. fusion, gemination or dens invaginatus could not be established. Although the presence of two canals may lead to diagnosis of fusion and the diagnosis of gemination can also be made, on the basis that tooth had only one root and there was no missing tooth. There was no grooves or if they may be they cannot be appreciated because of decomposition of the tooth surface over the cingulum area by caries. It is observed that in contrast to these anomalies, the crown of the tooth was almost normal in size mesio-distally, favoring the diagnosis of dens invaginatus but the other central incisor was normal in shape. Moreover, clinically cervical lingual groove and radiographically invagination of enamel to the interior of the root was observerved.
After all, the confusion still remains the same: fusion, gemination or dens invaginatus?
References
1. Rajendran R, Sivapathasundram B. Shafer’s textbook of oral pathology. Elseiver 7th edition;2012
2. Spatafore CM. Endodontic treatment of fused teeth. J Endodon 1992;18:628-31
3. Lowell RD, Solomon AL. Fused teeth. JADA 1964;68:762
4. Hülsmann M: Dens invaginatus: aetiology, classification, prevalence, diagnosis, and treatment considerations. Int Endod J 30: 79-90, 1997 .
5. Berman LH, Hartwell GR. Diagnosis. In: Cohen S, Hargreaves KM, Keiser K. eds. Pathways of the pulp, 9. edition, Mosby Elsevier. 2006: p, 2-39
6. Sawyer M, Peikoff MD, Trott JR. Endodontic therapy in an usual case of fusion. J Endodon 1980;6:796-8
7. Tsesis I, Steinbock N, Rosenborg E, Kaufman AY. Endodontic treatment of developmental anomalies in posterior teeth: treatment of geminated/fused teeth-report of two cases. Int Endodon J 2003;36:372-9
8. Itkin AB, Barr GS. Comprehensive management of the double tooth: report of case. JADA 1975;90:1269-72
|