Introduction
The prosthetic management of the edentulous patient has long been a major challenge for dentistry. For well over a century, complete maxillary and mandibular dentures have been the traditional standard of care. Most patients are not satisfied with the retention and stability of their complete dentures.[1] Whenever healthy roots are present, they should be retained and an attachment overdenture should be considered. Retained healthy roots, provide retention, support, and stability of the overdenture, preserves alveolar ridge height and maintain propioreceptive stimulus through periodontal membrane, economical and psychological benefits[2],[3],[4]. Such overdenture is capable of providing patients with a long duration of service and satisfaction. . For the prosthesis to be successful, all potential abutment teeth should be evaluated carefully for periodontal status, caries activity, potential for endodontic treatment and positional consideration. Healthy abutments must possess minimal mobility, adequate bone support at least 6mm and should be amenable to any periodontal treatment[2]. Broad band of attached gingiva is considered desirable for abutments. Patients with poor oral hygiene are considered poor candidates for root supported overdentures[2].
Successful endodontic treatment may provide favorable crown root ratio of abutments by reducing abutment crown to within 1mm of ridge crest. It also provides esthetic result by sufficient reduction of endodontically treated abutments and replacement with one of similar size and shape[2].
Determination of Position and number of retained abutment is of considerable importance for desirable overdenture. Two canines in one arch are most frequently considered treatment options. Since they have an adequate periodontal area, lie in strategic position in the arch and are amenable to endodontic treatment[2].
With accurate diagnosis, careful treatment planning, and patient compliance, root attachment overdenture have become an integral part of Prosthodontic treatment.
Zest Root Locator System
Root-supported overdentures attachments that are used to gain the retention and stability are simple connectors consisting of -One part that connects to the root and the other part to the overdenture acrylic denture base. Attachments are either resilient or nonresilient (rigid). A resilient attachment allows the prosthesis to have vertical, lateral, and hinging movements and 360 degree rotation at the attachment site as the patients chews. Up and down vertical movements helps the prosthesis to come in maximum contact of the mucosa and distribute the load over mucosa, away from abutment. While the 360 degree rotation at the attachment site allows greater load of distal mucosa and directs it away from the abutment. This action reduces the stress on the abutment tooth or implant. Only resilient attachments are used in the design of mucosal root-supported or implant-supported overdentures.[1],[6],[7],[8]
The Locator root-retained attachment (Zest Anchors) is classified as a Supraradicular, universal hinge, and resilient attachment for endodontically treated roots.
Indications
The Locator Root Attachment is designed for use with overdentures or partial dentures, retained in whole or in part by endodontically treated roots in the mandible or maxilla.
Stroke and arthritis patients are ideal candidates for this attachment.
Contraindications
Not appropriate where a totally rigid connection is required.
The Locator cannot be placed in mandibular incisor or lateral teeth or in maxillary lateral incisors.
When the supporting root structure is short or compromised
Features
Locating Design: Self Locating design allows a patient to easily seat their overdenture without the need for accurate alignment of the attachment components. It is designed with a locating skirt that seats the attachment in the proper location every time, regardless of the patient’s ability or dexterity. It is thus ideal for stroke patients or arthritis patients who have compromised dexterity and difficulty in exact overdenture placement.
Retention inside and outside: The unique Dual Retention innovation provides the Locator attachment with greater retention surface area than ever before available with other attachments. A combination of inside and outside retention ensures the longest lasting performance.
Choice of angles and retention: The LOCATOR attachment is an Supraradicular design which consists of the choice of a Direct Cement-in, Cast-to straight post and two angled (10º and 20º) to accommodate divergent roots. Three different retentive males allow for your choice of regular, heavy, or extra-heavy retention according to the needs of the patient.
Rotational pivoting action: The design of the pivoting LOCATOR male allows a resilient connection for the prosthesis without any resulting loss of retention. The retentive nylon male remains completely in contact with the female socket while its metal denture cap as a full range of rotation movement over the male
Core Insertion / Removal Tool: The plastic males are easily removed from the metal housing and replaced using the Locator Core Insertion / Removal Tool.
Technique for placement of the Locator female in natural teeth for Direct technique
Complete the endodontic procedures and decoronate the root surface occlusally to within 1.0 mm supragingivally.
The LOCATOR requires at least 4mm root diameter. Plastic Depth Reference Ring are Set on the Pilot Drill to a depth slightly exceeding the length of the female post (approx 7mm). Irrigation is recommended to prevent overheating. The root surface is countersunk using the Spot Facer (Countersink Diamond Bur) to a depth where a full 360 degree recessed seat appears on the occlusal surface of the root. When making the countersink preparation into a divergent root, the depth of the countersink will vary across the surface of the root. On the shallow side of the preparation, create a minimal recessed seat using the Spot Facer.
A portion of the original depth from the Pilot Drill canal preparation will be lost due to countersinking. Re-establish the full depth of the canal preparation by re-preparing with the Pilot Drill using the original Depth Reference Ring setting.
Note: Care should be taken not to countersink excessively with the Spot Facer. The majority of the occlusal aspect of the LOCATOR female must remain above the face of the root to allow the male to snap in without interference. Now using the Locator Parallel Post as a handle, place a 0 Degree Female into the completed preparation to visually approve proper fit and parallel alignment of the attachment. If alignment of the attachment can be improved, select the most suitable angled female (10 or 20 degrees) and rotate it in the canal to determine its orientation to make parallel.
Note: Create a small indexing mark on the female base and the root surface to help return the angled female to the exact position during cementation.
Cement the LOCATOR Female in place with composite resin cement, lining up index mark. After the cement has set, round off and polish the root surface to remove excessive cement around female. The Parallel Post can be placed over the female to protect it during the polishing.
Place a White Block-Out Spacer over the head of cemented female. The spacer is used to block out the remaining exposed surfaces of the root. Insert a LOCATOR Black Processing Male with metal housing into cemented female, leaving the White Block-Out Spacer beneath it. The Black Processing Male will maintain the overdenture in the upper limit of its vertical resiliency during the processing procedure. Prepare a recess in the denture to accommodate the protruding Processing Male. Make a small vent hole on the lingual aspect to express excess resin. Verify that adequate space has been provided for the stainless steel housing before curing. Apply a small amount of self-curing acrylic around the housing of the Processing Male, and in the recess of the denture. Ask patient to close in light occlusion until acrylic sets.
Use the LOCATOR Male Removal Tool to remove the Male Inserts from the metal denture cap. The LOCATOR Male Insertion Tool is used to firmly push a LOCATOR Replacement Male into the empty metal denture cap. The replacement male must seat securely into place, level with the rim of the cap. Locator male attachments are available in varying amounts of retention. The black male attachment provides the least amount of retention at 1.0 pound; the pink male attachment provides 3.0 pounds of retention; and the white male attachment provides 5.0 pounds of retention and is considered the regular or standard for this system. With two to four abutment teeth, the maximum retention should be used (the white male at 5.0 pounds per attachment). If more than four abutments are used, any combination of black, pink, and white attachments can be used to create the maximum retention for the overdenture (20 pounds is ideal). If there is too much retention with these attachments the overdenture cannot be removed easily. Choose the final Locator nylon retention liner based upon the maximum amount of retention needed to retain the overdenture.
Give patient instructions on placement and removal of the overdenture .Oral hygiene instructions are given. Overdenture abutments should be brushed at least once a day with gel toothpaste to remove plaque and to stimulate gingival tissues. On each exposed root surface, daily application of 1.1% neutral sodium fluoride or 0.5% stannous fluoride is advisable. Poor oral hygiene has the potential for root or implant failure in overdenture cases.[9]
Case No 1
The 63 years old female patient presented with carious tooth structure around the amalgam overdenture abutments on two mandibular canines and the right mandibular second bicuspid. The residual maxillary ridge mucosa was healthy. Extraoral examination revealed reduced vertical dimension of the face and unsupported lips. The patient was satisfied with the esthetics of preexisting denture. The patient expressed a strong desire to keep his roots and avoid surgery. Decay was removed from the cuspid roots but the second bicuspid was not restorable and subsequently extracted. The panoramic radiograph demonstrated previous successful endodontic therapy and sufficient root structure in the bone and periodontally sounds canines. The proposed treatment included maxillary conventional denture and mandibular overdenture retained with Zest root locator attachment in a direct technique on bilateral mandibular canines. The patient was quite pleased with the retention of the denture. (Fig 1 to 10).
 | Fig 1 : Picture showing decoronation of the cuspids and completed endodontic treatment of the same.
 |
 | Fig 2 : Picture showing spot-faced bur being used to create an internal dentinal seat for the Locator female post.
|
 | Fig 3 : Picture showing placement of positioning pins for checking parallelism of the Locator female.
|
 | Fig 4 : Picture showing cemented Female Root Locators in the cuspid.
|
 | Fig 5 : Picture showing white block-out spacer placed over the head of each cemented Locator female.
|
 | Fig 6 : Picture showing Titanium cap with black low density polyethelyne male inserted into each cemented female, leaving the White block-out spacer beneath it.
|
 | Fig 7 : Picture showing the polished denture after removing the excessive acrylic which had flown around the titanium cap.
|
 | Fig 8 : Picture showing the black processing male Locator which has been removed from the titanium cap Photo
|
 | Fig 9 : Picture showing Nylon Male Locator inserted in the Titanium housing
|
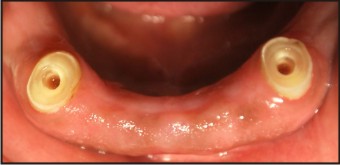
 | Fig 10 : Post Operative with denture in place
|
Case No 2
A 35-year-old man reported with the chief complaint of missing lower and few upper teeth. Intraoral examination revealed the presence of 13, 14, 15, 23, 24 teeth and partially edentulous mandibular arch with presence of anterior teeth. The mandibular anterior teeth showed marginal bone loss around them. The treatment plan was extraction of teeth No.14, 15, 24 and a bone graft on all extraction sites for possible future implant considerations.
A barrier memberane was placed on the grafted sited. 13 and 23 were found to be healthy with adequate bone support. A temporary acrylic denture was used to replace the missing teeth. Endodontic therapy was performed on teeth No. 13 and 23. The teeth were decoronated to within 1.0mm of the gingival crest and the Zest Locator attachment system for overdenture was cemented with the help of self adhesive cement into each root. The patient was extremely satisfied with the retention of the denture and to have avoided extraction of his remaining cuspid roots, maintaining sensory inputs. (Fig 11 - 17).
 | Fig 11 : Pre Operative situation
|
 | Fig 12 : Picture showing decoronation of the cuspids and completed endodontic treatment of the same
|
 | Fig 13 : Picture showing placement of positioning pins for checking parallelism of the Locator female.
|
 | Fig 14 : Picture showing cemented Female Root Locators in the cuspid.
|
 | Fig 15 : Picture showing cemented Female Root Locators in the cuspid.
|
 | Fig 16 : Picture showing white block-out spacer placed over the head of each cemented Locator femal
|
 | Fig 17 : The final denture with Zest anchor Male attachments
|
Discussion
Complete denture retention has always been a challenge. To overcome the problems associated with conventional complete dentures the use of overdentures with attachment has become an integral part of prosthodontic treatment. Complete diagnosis and treatment planning are most important for the success of overdentures. Root supported overdenture provides alternative treatment to extraction of natural teeth and completes dentures provides the patient with greater retention, stability, and comfort and improved function, esthetics, and phonetics. The Locator attachment is designed for patients who have difficulty seating their overdentures. Stroke and arthritis patients are ideal candidates for this attachment. Another advantage of such attachment is dual retention and the design of the pivoting LOCATOR Male which allows a resilient connection for the prosthesis without any resulting loss of retention. The technique for constructing root-supported overdentures can easily be constructed within the skill level of most general dentist.
Conclusion
With Complete diagnosis, treatment planning and patient compliance the overdenture has been a proven mainstay of conservative prosthodontic treatment. This treatment modality preserves residual ridge by retaining teeth or roots which in any case cannot be used for removable partial denture or as fixed partial denture abutments but are useful to support an overdenture. Thus By satisfying patient’s wish for a conservative treatment and providing the above advantages of using Locator attachments, enhanced retention and stability can be achieved. This again contributes to increase in comfort, function, esthetics, phonetics and promote a healthy oral environment.
Refrences
1. Pavlatos J. Root-supported overdentures. CDS Rev 1998;9 1:20-25
2. Morrow RM. Handbook of immediate overdentures. St. Louis: Mosby; 1978:48.
3. Castleberry DJ. Philosophies and principles of removable partial overdentures. Dent Clin North Am 1990; 34:589-592.
4. Renner RP. The overdenture concept. Dent Clin North Am 1990; 34:593-606.
5. Pavlatos J. The root-supported overdenture using the Locator overdenture attachment. CDS Rev 1997;90:32-9
6. Pavlatos J. Mandibular implant-supported overdentures. CDS Rev 1997; 90:32-39.
7. Sterngold/Implamed. Procedure manual. Sterngold; 1998:3.1-4.
8. Staubli P. Attachments and implants reference manual, ed. 6. San Mateo, CA: Attachments International;1999:1-9
9. Terracciano-Mortilla L. Prosthodontics and maintenance for dental auxiliaries. Implant News Views 2000;2:4
|