Introduction:
Facial defects can cause not only functional problems but also some serious psychological problems that can cause the individual to avoid social stigma[1]. Auricular defects may be congenital or acquired and are the second most common craniofacial malformation after cleft lip and palate. There are two main treatment options namely surgical reconstruction and using auricular prosthesis. The former is a great challenge to surgeons because of the complex shape and size of the human ear. On the other hand, rehabilitation with a prosthetic ear which is matched to the contra-lateral ear provides a better morphologic result[2]. In the present case, retention of auricular prostheses was provided by eyeglass. Heat polymerizing acrylic resin auricular prosthesis provides promising outcome within the limitation of the material. Successful outcome is completely dependent on the prosthodontist’s skill and expertise. The purpose of this article is to present a technique for fabricating heat polymerizing acrylic resin auricular prosthesis retained by eyeglasses.
Case Report:
A 27 year old male patient, reported to the Department of Prosthodontics, Government Dental College,Trivandrum with the chief complaint of congenitally missing right external ear. On general examination it was found that patient’s right ear was aplastic and the left ear was normal in appearance with normal hearing pattern in both the ears. There were no associated features suggestive of microtia or any other syndrome. Patient was devoid of any other systemic disorders and the family history was found to be irrelevent.
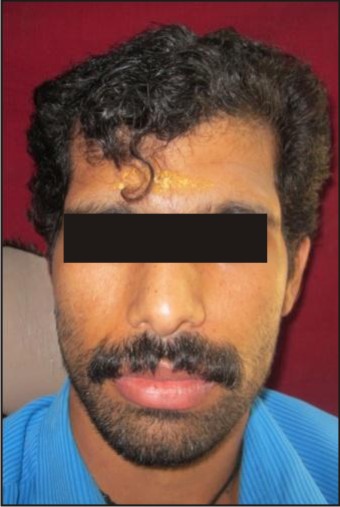 | Fig : 1 Pre-operative view
 |
 | Fig : 2 Post-operative view
|
 | Fig : 3 Alginate impression of doner ear
|
 | Fig : 4 Wax pattern adaptation over the defect region
|
 | Fig : 5 Wax pattern check up
|
 | Fig : 6 Three pour technique
|
 | Fig : 7 Prosthesis try-in
|
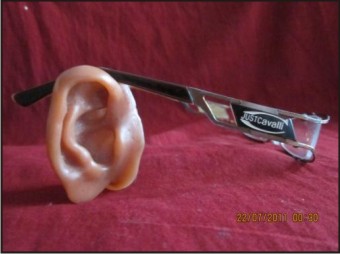 | Fig : 8 Eyeglass retained prosthesis
|
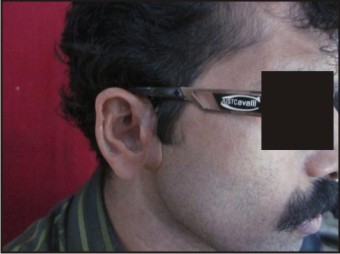 | Fig : 9 Prosthesis in position
|
Procedure:
Impression of the auricular defect was made with irreversible hydrocolloid impression material (ALGIPLAST, INDIA PVT.) after the hair adjacent to the defect area was coated with petroleum jelly (Vaseline; Chesebrough-Pond’s USA Co). Impression material was then supported with plaster of paris. After removal, the impression was boxed and poured in dental stone (Type III). An ear pattern was created using the ‘‘donor technique,’’ in which a relative or a person with ear contours that closely mimic those of the patient acts as the donor to make an ear impression[1]. Hair adjacent to the right ear was coated with petroleum jelly and ear impression was made with irreversible hydrocolloid impression material supported by plaster of paris. After setting, it was carefully removed and inspected for any deficiencies or inaccuracies. The ear impression was poured in molten modelling wax (ROLEX, DENTAL PRODUCT, DELHI) to form a positive replica of the right ear. A wax pattern for the right ear was modified to the desired morphology corresponding to the patient’s left ear.
After proper positioning of the wax pattern on the defect, the boundary of waxed ear was outlined with the gentian violet on the patient’s facial skin and is oriented in symmetry to the left ear .This outline was replicated on the cast of defect impression for the purpose of proper adaptation of wax pattern. The prepared wax pattern was adapted onto the stone model and then it was checked for accuracy of fit and esthetic on the patient’s face.
The wax pattern was invested in a dental flask using three pour technique. Routine wax elimination was done. After the complete removal of wax, the heat polymerizing acrylic resin which was intrinsically coloured using pigments according to the patient’s skin colour (Intrinsic Coloring Kit Factor II, Lakeside, USA) was packed in dough stage. The material was processed according to the manufacturer’s direction. Processed prosthesis was removed and polished.
The eyeglass of proper fit was selected and then the polished auricular prosthesis was attached to the eye glass with autopolymerizing resin in the desired orientation and adaptation. The prosthesis was placed on to the patient face and found to be harmoniously matching the normal side of the face in proper dimension and shape. The anatomic contour of the auricular prosthesis was quite similar to those of the normal ear as well. Instructions about care of the prosthesis were given. Recall visit of 1 week, 1month and 6 months was followed and found that patient was satisfied with the given prosthesis.
Discussion:
Maxillofacial defects can keep the patient away from normal daily activities of the life. Many patients with these defects have been rehabilitated successfully with prosthetic restorations. Secondary mechanical factors such as tissue undercuts, skin adhesives[3] and implants can provide retention[1]. The use of craniofacial implants (mastoid) for retention of extraoral prosthesis such as ears offers excellent support and retentive abilities. The bar-clip system and magnets provides good retention in implant supported auricular prostheses[5]. However, bars may limit access for performing hygiene procedures and make it difficult to insert and remove the prosthesis and also the magnets get deteriorated with time.
In the present case a non-surgical reconstruction of right auricular defect was chosen keeping in mind the patient’s financial status. Moreover, patient was not willing for invasive implant surgery. In the patient’s present situation there was no undercuts to hold the prosthesis in position, hence eyeglass retention was planned[4]. Heat polymerizing acrylic resin auricular prosthesis was selected over the silicone because of their dimensional and colour stability. It was found to be more economic as well. In the fabrication of the prosthesis, three pour techniques were followed for the easy retrieval of prosthesis without fracture. Advantages of eyeglass retained auricular prostheses are the ease in insertion and removal and also better maintainance.
The procedure suggested in the case report provides an alternative treatment option to the implant retained auricular prosthesis which improves the patient’s appearance and quality of life.
References:
1. A. Nilgun Ozturk, Aslihan Usumez, Zekeriya Tosun. Implant-Retained Auricular Prosthesis: A Case Report (Eur J Dent 2010;4:71-74).
2. Ting Jiao, Fuqiang Zhang, Xuemei Huang, Chengtao Wang. Design and Fabrication of Auricular Prostheses by CAD/CAM System (The International Journal of Prosthodontics, Number 4, 2004 Volume 17).
3. Holgers KM, Tjellstrom A, Bjursten LM, Erlandsson BE. Soft tissue reaction around percutaneous implants: A clinical study on skin penetrating titanium implants used for bone-anchored auricular prostheses.( Int J Oral Maxillofac Implants 1987;2:35–39.)
4. Hooper SM, Westcott T, Evans PLL, Bocca AP, Jagger DC. Implant supported facial prostheses provided by a maxillofacial unit in a UK regional hospital: Longevity and patient opinions.( J Prosthodont 2005;14:32–37.).
5. Chung RWC, Siu ASC, Chu FCS, Chow TW. Magnet-retained auricular prosthesis with an implant supported composite bar: (A clinical report. J Prosthet Dent 2003;89:446–449.)
|