Introduction
Dental plaque is a sticky, soft, colorless material adhering to the teeth, consists of bacterial cells (60-70% the volume of the plaque), salivary polymers, food residuals and bacterial by-products. Dental plaque is redefined as naturally-constructed biofilm. In addition to the bacterial cells, plaque contains a small number of epithelial cells, leukocytes, and macrophages. Bacteria that live in the mouth thrive on foods producing acidic metabolites[1]. Over a period of time, these acids destroy the tooth enamel, resulting in tooth decay. The acids that cause tooth demineralization (cavity formation) are produced by specific types of bacteria, which may helps to colonize leads to formation of plaque. The Bacteria that cause tooth decay utilize sugars as their food source[2]. The waste products created from digesting these sugars are the acids especially lactic acid cause the demineralization of tooth enamel and the dentin. The cells are contained within an extracellular matrix, which is formed from bacterial products and saliva. The extracellular matrix contains protein, polysaccharide and lipids. Inorganic components are also found in dental plaque; largely calcium and phosphorus which are primarily derived from saliva[3],[4],[5]. The inorganic content of plaque is greatly increased with the development of calculus. The practical consequences of calculus formation are that the deposit is significantly more difficult to remove once calcified, and it leaves a rough surface on the root which is easily colonized by plaque. Dental plaque is also the cause of periodontal diseases, which are bacterial infections that affect the supporting structures of the teeth. The most frequent form, gingivitis, is an inflammatory condition of the gums, associated with accumulations of bacterial plaque in the area[6],[7],[8]. Diseases that are confined to the gum usually do not lead to loss of teeth, but there are other more serious forms of periodontal disease that affect deeper tissues including bone. Plaque bacteria in these infections are very complex populations, which can enter the gums and stimulate irreversible destruction of surrounding tissues. Plaque inhibition can be achieved by natural products instead of using chemicals to avoid side effects.
Anti-plaque and anti-gingivitis properties of tea decoction are considered along with their substantivity, safety and possible clinical usefulness by natural products. Green tea is considered a dietary source of antioxidant nutrients: green tea is rich in polyphenols (catechins and gallic acid, particularly), but it also contains carotenoids, tocopherols, ascorbic acid (vitamin C), minerals such as Cr, Mn, Se or Zn, and certain phytochemical compounds[9]. These compounds could increase the GTP antioxidant potential which will decrease the acidic conditions of plaque results in recovery from the dental diseases.
The aim of this study was to evaluate plaque inhibitory agents in mouthwashes used to inhibit bacterial plaque formation and thus to prevent or resolve chronic gingivitis, can only affect supragingival plaque. We tested significance of tea decoction mouth rinse on dental plaque among the school childrens.
Research Methodology
Approach and Design
The research approach adopted was quasi-experimental to achieve the objectives of the study. The research design selected for the present study is “pre-assessment and post-assessment for the Experimental and control group based on the index score screening of the sample and significance of the mouth rinse drawn from Cronbachs Alpha method[10], [11].
Population and Sample preparation
The selected population to this study comprise of school children (6-12 years) from Govt. Municipal Corporation Upper Primary School, Tirupati. The sample prepared with 30 school children in experimental group and 30 school children in control group, who fulfill inclusion criteria as follows: i) in the age group of 6-12 years ii) Not associated with oral lesions and ulcers.
Dental Examination
Apply the plaque disclosing solution to the surface of the tooth and determine the plaque index score by the formulae (maxillary right first molar + maxillary right lateral incisor + maxillary left first bicuspid + Mandibular left first molar + Mandibular left lateral incisor + Mandibular right bicuspid) /6 and Suggested nominal scale for individual evaluation: Excellent -0, Good- 0.1 – 0.9, Fair- 1.0 – 1.9, Poor - 2.0 – 3.0 (Table-1) [12]. The pre-assessment was done in experimental and control groups before providing tea decoction mouth rinse intervention. This intervention was provided for three minutes to the experimental group school children while control group school children did not receive tea decoction intervention. After 7 days post-assessment was done in experimental and control group school children.
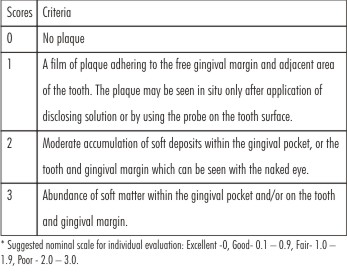 | Table 1: Screening Of The Individual Using The Plaque Index Score On The Teeth
 |
Content Validity and Data Analyses
The content validity of the tool was obtained from nursing and medical experts. The content validity of the tool was given to 10 experts along with the objectives of the study. There were 5 experts in the field of Nursing and 2 experts in the field of Pediatric Medicine and 3 experts in the field of Dental Medicine; the experts were requested to give their opinion on relevance and appropriateness of the tool. According to their suggestions, modifications were made in the tool. The modified tool was used for the study. Analysis of data was done using descriptive and inferential statistics. The analysis of data showed that there was significant difference between pre and post assessment with t-value of 17.031 (t table value is 2.94) and this difference was significant at 0.01 level. The findings of the study showed that the tool was reliable and feasible to conduct the study. The reliability was established by “Cronbachs Alpha” method.
Interpretation and Discussion
In the present study the distribution of level of dental plaque index among experimental and control group school children in pre and post-assessments are presented in (Table-2) shows that out of 30 school children in experimental group 0% had excellent dental plaque index, 30% had good dental plaque index, 33 % had fair dental plaque index and 36% had poor dental plaque index respectively. Where as in control group, out of 30 school children 0% had excellent dental plaque index, 0% had good dental plaque index, 40% had fair dental plaque index and 60% had poor dental plaque index respectively. The overall dental plaque index among school children in pre-assessment reveals that majority i e; 48% had poor dental plaque index, 36% had fair dental plaque index, 15% had good dental plaque index and 0% had excellent dental plaque index respectively and in Post-assessment are presented in (Table-3) shows in control group, out of 30 school children 0% had excellent dental plaque index, 0% had good dental plaque index, 13.33% had fair dental plaque index, and 86.67% had poor dental plaque index respectively. Overall dental plaque index among school children in post-assessment reveal that a majority 46% had poor dental plaque index, 11% had fair dental plaque index, 23% had good dental plaque index and 18% had excellent dental plaque index respectively.
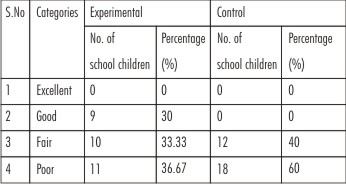 | Table-2: Level Of Dental Plaque Index Among Experimental And Control Group School Children In Pre-assessment.
|
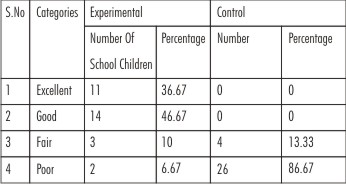 | Table-3: Level Of Dental Plaque Index Among Experimental And Control Group School Children In Post-assessment.
|
The Effectiveness of tea decoction mouth rinse on dental plaque in experimental and control groups shows that in experimental group, the mean value of dental plaque index in pre assessment was higher (mean = 1.598, S.D = 0.655) than in post assessment (mean = 0.289, S.D = 0.548) (Table-4). The obtained paired‘t’ value was 14.091 (p<0.01), which was highly significant at one per cent level. This clearly shows that there is a significant difference in the dental plaque index among school children before and after performing tea decoction mouth rinse. Tea decoction mouth rinse is therefore highly effective in reducing dental plaque among school children. In control group, the obtained mean value of dental plaque index in post assessment was higher (Mean = 2.007, S.D = 0.204) than in pre assessment (Mean = 1.976, S.D = 0.194) (Table-5). The obtained‘t’ value was 1.065, which was not significant. This clearly shows that there is a significant increase in the dental plaque index among school children in post-assessment than pre assessment (Figure 1). It indicates that there was a significant reduction in levels of dental plaque index in experimental group. Whereas, in control group, there was no significant reduction in the levels of dental plaque index, which shows the effectiveness of tea decoction mouth rinse on dental plaque. Comparatively the effect of tea decoction mouth rinse on dental plaque between experimental and control group school children shows that in pre-assessment the mean dental plaque index was 1.598 with S.D 0.655 in experimental group and it was 1.976 with S.D 0.194 in control group and the student ‘t’ test value obtained was 0.66, which is statistically not significant. In post-assessment the mean dental plaque index was 0.289 with S.D 0.548 in experimental group and it was 2.007 with S.D 0.204 in control group and the student ‘t’ test value obtained was 16.108, which is statistically significant at one per cent level (data not shown).
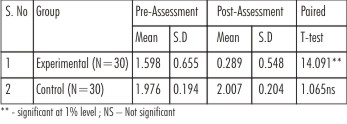 | Table-4: Pre-assessment And Post-assessment Mean, Standard Deviation And Paired T-value Of The Dental Plaque Index Among School Children In Experimental And Control Groups.
|
 | Table-5: Mean, Standard Deviation And Student ‘t’ Test Value To Compare Dental Plaque Index Between Experimental And Control Group School Children.
|
The results show that there was no significant difference in dental plaque index in pre mouth rinse assessment between experimental and control groups. There was significant difference in dental plaque index in post mouth rinse assessment between experimental and control groups (Figure 1 & 2). It indicates that after tea decoction mouth rinse the dental plaque reduced significantly when compared to pre mouth rinse assessment, this supports that tea decoction mouth rinse is effective in reducing the dental plaque among school children.
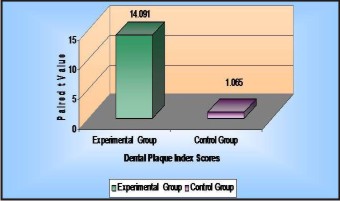 | Figure-1 : Distribution Of Paired ‘t’ Test Scores Of Dental Plaque Index In Experimental And Control Groups.
|
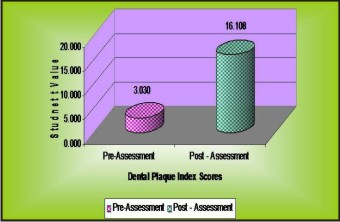 | Figure-2 : Distribution Of Student ‘t’ Test Scores Of Dental Plaque Index Among School Children
|
References
1. Cheng, L.; Weir, M. D.; Xu, H. H.; Antonucci, J. M.; Lin, N. J.; Lin-Gibson, S.; Xu, S. M.; Zhou, X. J Biomed Mater Res B Appl Biomater 2012, doi: 10.1002/jbm.b.32709.
2. Touger-Decker, R.; Vanloveren, C. Am J Clin Nutr 2003, 78, 881S-892S.
3. Jin, Y.; Yip, H. K. formation and control. Crit Rev Oral Biol Med 2002, 13(5), 426-441.
4. Nancollas, G. H.; Johnsson, M. A. Adv Dent Res, 1994, 8(2), 307-311.
5. Barone, J. P.; Nancollas, G.H. J Dent Res 1978, 57(1), 153-161.
6. Benakanakere, M.; Kinane, D. F. Front Oral Biol, 1978, 15, 41-55.
7. Ebersole, J.L.; Cappelli, D.; Holt, SC.; Singer, RE.; Filloon, T. Oral Microbiol Immunol. 2000, 15(1), 19-26.
8. Gangadhar, V.; Ramesh, A.; Thomas, B. Indian J Dent Res, 2011, 22(4), 537-541.
9. Eley, B. M. Br Dent J, 1999, 186(6), 286-296.
10. Yu, C.H. Proceedings of the 26th SAS User Group International Conference, 2001, 1-7.
11. Santos, J.R. 1999, 37(2). Available at: http://www.joe.org/joe/1999april/tt3.html
12. Blinkhorn, A.; Choi, C.; Paget, H. Eur J Dent Educ , 1998, 2 (1), 39–41.
|