Introduction
A considerable amount of work has been done on oral sensation and perception in the past few years.[1],[2],[3],[4] Oral stereognosis is the phenomenon by which the size and form of objects is determined in the mouth. This has attracted greater attention as compared to the studies on the threshold of taste among denture wearers and non-denture wearers.
Taste as we ordinarily think of it, is dependent upon a number of factors and these are the foods solubility, smell, temperature as well as the type and intensity of a combination of taste quality.
Purpose And Rationale Of Study
A number of psycho-physiologic factors interact to determine what will be the reaction of a denture wearer to his complete dentures. They may express their requirements for mastication, deglutition, speech and esthetics. However, sensory perception, especially to the effect of dentures on taste, olfaction and oral tactile sensitivity has often been overlooked.
Hence, this study was conducted to determine the influence of using different denture base materials on the taste thresholds of denture wearers.
Materials And Methods
5 dentulous subjects of 25-30 years old were selected. 3 subjects had no history of pertinent medical involvement and were receiving no medications. 4 maxillary dentures, differing only in their palatal surface topography and material were needed for the study of each patient. Following were the denture surfaces and material types:
Palatal plate 1: acrylic resin denture with smooth palatal surfaces.
Palatal plate 2: acrylic resin denture with simulated rugae pattern.
Palatal plate 3: cast metal polished palatal surface.
Palatal plate 4: cast metal polished corrugated palatal surface.
The plate thickness of each denture was kept at 1.5mm.
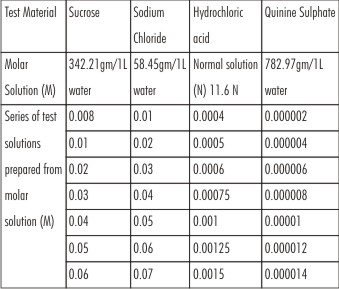
Gustatory sensitivity was assessed by means of the taste test with the help of the syringes containing 7 different concentrations of four taste qualities. These were placed on the anterior two-thirds of the patient’s tongue.
The tests were done before and after insertion of the four different dentures. The patient could identify or percept different taste modalities and his response was noted.
The test materials and solutions were used in accordance with the average adult values of taste threshold given by Keele and Neil.[5]
 |
 |
Results
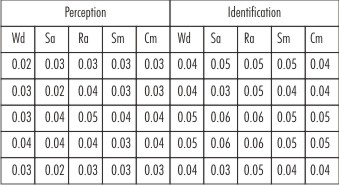
The results obtained are tabulated below (Tables 1 to 5). The sweet and sour test materials might have increased the palatal salivary flow resulting in increased perception and identification of these tastes as compared to salt and bitter test materials. These findings concur with the findings of Kapur et.al wherein it was reported that stimulated salivary flow increased in denture wearing.[7]
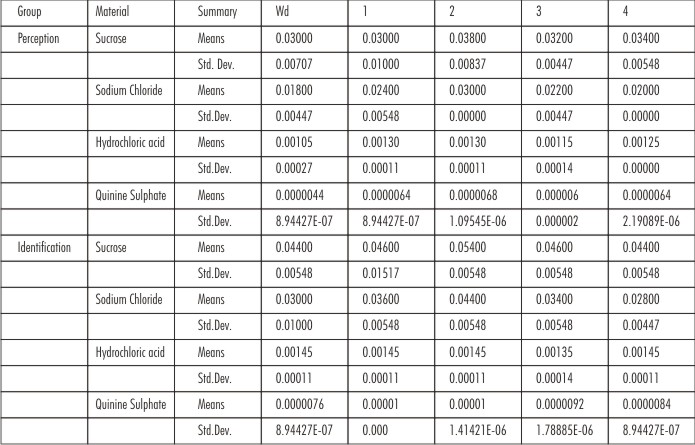 | Table 1: Summary Table
|
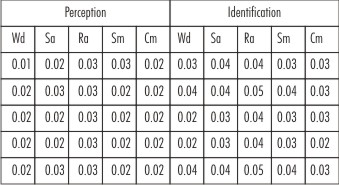
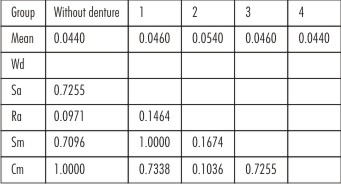
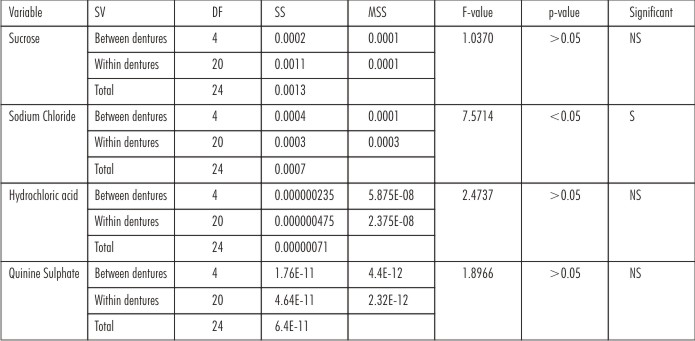 | Table 2: Comparison Of Dentures With Respect To Perception Scores
|
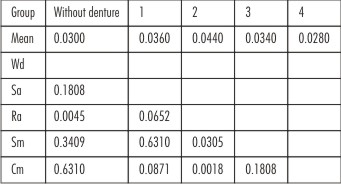
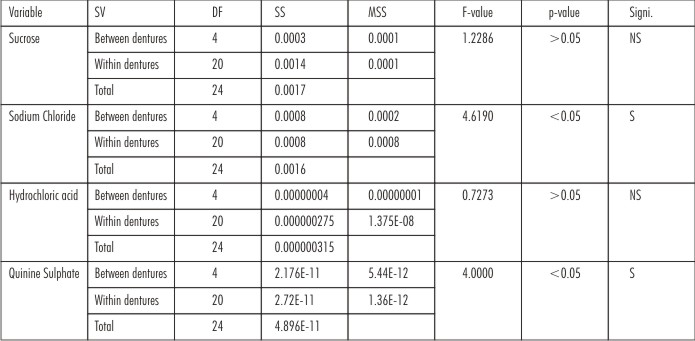 | Table 3: Comparison Of Dentures With Respect To Identification Scores
|
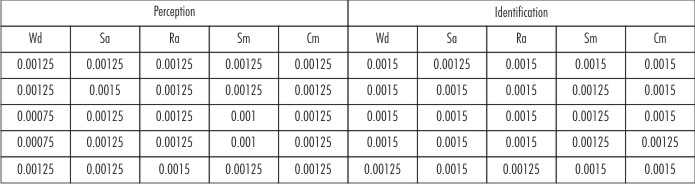
 | Table 4(A): Sucrose Test Values For 5 Patients
|
 | Table 4(B): Sodium Chloride Test Values For 5 Patients
|
 | Table 4 ( C ): Hydrochloric Acid Test Values For 5 Patients
|
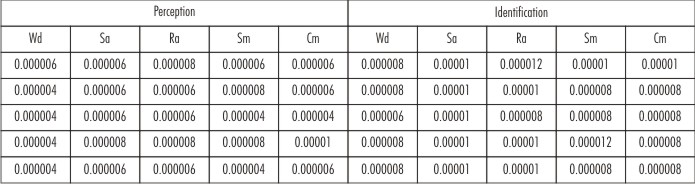 | Table 4 ( D ): Quinine Sulphate Test Values For 5 Patients
|
 | Table 5 ( A ): Duncan Multiple Comparison Test Procedure-sucrose
|
 | Table 5 ( B ): Duncan Multiple Comparison Test Procedure-sodium Chloride
|
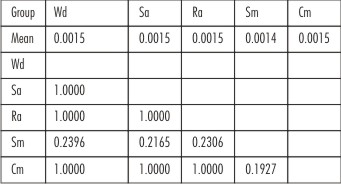 | Table 5 ( C ): Duncan Multiple Comparison Test Procedure-hydrochloric Acid And Quinine Sulphate
|
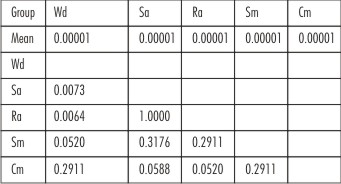 | Table 5 ( D ): Duncan Multiple Comparison Test Procedure-hydrochloric Acid And Quinine Sulphate
|
It may be observed that all the subjects could specifically point out to both stages of taste threshold for each modality with or without palatal plates. It is further observed that the identification threshold was at a little higher level of concentration than perception for all the four modalities of taste. The mean perception and identification values were subjected to statistical analysis. It was proved that the difference between perception and identification threshold was highly significant.
Discussion
The present investigation was undertaken to explore the validity of a very common observation that complete dentures adversely affect the taste sense. Kumamato et al. were of the view that more covered is the palate, lesser is the taste as well as the stereognostic ability.[3]
A variety of taste receptors have been identified such as- ion channels, ligand-gated channels, enzyme and G-protein coupled receptors (GPCRs). Certain sub-types of taste receptors within a taste quality are predominately located in one region of the tongue, making it more sensitive but not exclusive to a taste quality. It is observed that different basic tastes have different ionic mechanisms. Most types of gustatory stimuli fall under the water soluble and non-volatile type and only some are lipophilic type, example being the bitter tasting quinine and caffeine. As a result of this investigation, it was found that all the subjects could specifically point out to two stages of threshold – one for perception and one for identification of taste. This was so in case of each modality of taste and also with or without the dentures in the mouth. The same finding was reported by other authors as well.[4],[6],[7]
Salt taste: Salty taste is produced by monovalent cations like Na+ and K+ and the chloride anion, Cl-, inhibits the cation. Larger the anion, greater is the taste inhibition of the cation. As the anions get larger, they take on a bitter or even a sweet taste. Although the presence or absence of a palatal plate did not make a statistically significant difference on the hydrochloric acid or sucrose group, the results were significant for the quinine sulphate and sodium chloride group. Both the identification as well as taste perception was statistically significant for sodium chloride and for quinine sulphate, only the identification was statistically significant.
It can be perceived that the resin denture plates do not help identify or perceive lower concentrations of salt as a result of which, complete denture wearers require higher concentrations of salt in their food preparations. For metal dentures, it was found that double the concentration of salt was required for identification and perception.
Sour taste: Virtually all acids taste sour which is mediated by protons (H+) having a local effect on oral soft and hard structures.
Sweet and bitter taste: This category of taste sensation is mediated by organic compounds. Carbohydrates and amino acids are sweet tasting, whereas alkaloids, certain divalent cations and few other amino acids are bitter tasting. Denatonium is the bitterest substance known to man.
Clinical Implications
It can be observed that in the initial stages, the patient could not perceive the taste of salt.
However based on this study it is recommended that dentures should be palatal rugae pattern than making it conventionally smooth.
Limitations Of The Study
Small sample size and young subjects as compared to elder denture wearer group were selected. This might have resulted in smaller concentration of different taste materials especially sweet (sucrose) and sour (hydrochloric acid) tastes. The location of taste material on the tip of the tongue and side of the tongue also might have resulted in disbursement of the solution and variation in observations. It has been observed that taste varies with health, attitude, hunger and even food temperature. There is a gradual shift of taste from the tip of the tongue to the circumvallate papillae. Sweet taste is most prominent at the tip of the tongue and as we proceed posteriorly, perception of salty taste diminishes and sour taste becomes more prominent.
Summary And Conclusion
On the basis of the findings discussed, the following conclusions have been drawn:
1. All the subjects exhibited two taste thresholds, one perception threshold when they detected the test solution but could not identify the taste correctly, and an identification threshold when they could identify the specific taste also.
2. Both the perception and identification thresholds for each taste modality seemed to be considerably increased immediately after the insertion of the palatal plates. For perception and identification, this increase was found to be the highest for sodium chloride and for quinine sulphate, for identification only. The presence or absence of a palatal plate did not make a statistically significant difference on the hydrochloric acid or sucrose group.
3. Metal denture plates required double the concentration of taste modalities as compared to the resin plates.
4. However, rugae pattern resin plates and corrugated metal plates could perceive taste better than conventional smooth pattern resin or metal plates.
References
1. Litvak H, Silverman SI, Garfinkel L. Oral stereognosis in dentulous and edentulous subjects.J Prosthet Dent 1971; 25(2):139-151.
2. Strain JC. The effect of complete dentures on taste perception. J Prosthet Dent 1952;2(1):60-67.
3. Kumamato Y, Kaiba Y, Imamura S, Minakuchi S. Journal of Prosthodontic Research 2010;54(2):92-96.
4. Murphy WM. The effect of complete dentures on taste perception. Br Dent J 1971; 130:201-205.
5. Keele CA, Neil E. Samson Wright’s applied physiology. Oxford University Press. 1971.
6. Henkin RI, Christiansen RI. Taste localization on the tongue and pharynx of normal man. J App Physiol 1967; 22 (2):316-320.
7. Kapur KK, Collister T, Fisher EE. Masticatory and gustatory salivary reflex secretion rates and taste thresholds of denture wearers. J Prosthet Dent 1967; 18:406-416.
8. Van Aken AA, Van Waa S, Kalk W. Int J Prosthodont 1991;4(1):75-79.
9. Smith PW, McCord JF. Oral stereognostic ability in edentulous and dentate individuals. Eur J Prosthodont Restor Dent. 2002; 10:53–6.
10. Mantecchini.G, Bassi.F, Pera.P, Preti.G. Oral stereognosis in edentulous subjects rehabilitated with complete removable denture. J Oral Rehabil 1998; 25; 185-9.
11. Berry DC, Mahood M. Oral stereognosis and oral ability in relation to prosthetic treatment. J Prosthet Dent 1966; 15:179.
12. Chauvin JO, Bessette RW. Oral stereognosis as a clinical index. New York State Dental Journal 1979; 40:543.
13. Crum RJ, Losielle RJ. Oral perception and proprioception: A review of literature and its significance to prosthodontics. J Prosthet Dent 1972; 28:215.
14. Jacobs R, Bou Serhal C, van Steenberghe D. Oral stereognosis: a review of the literature. Clin Oral Investig. 1998; 2:3–10.
|