Introduction
Root canal therapy requires a thorough knowledge of root canal morphology to adequately clean and shape the canal system. It is generally recognized that the incomplete instrumentation and cleaning of root canals will lead to endodontic failure. Frequently root canals are left untreated because the clinicians fail to identify their presence, particularly in teeth that have anatomical variations or additional root canals (Slowey 1979), before the root canal treatment is performed. Therefore, the clinician should be aware of the configuration of the pulp space of the tooth that is to be treated.
As a group, the mandibular premolars are very difficult to treat; they have a high flareup and failure rate. A possible explanation may be the extreme variations in root canal morphology in these teeth i.e. frequent existence of an extra canal. The bifurcation of second canal may occur in the mesiodistal dimension or the buccolingual dimension and in different levels of the roots. Sudden narrowing or disappearance of the root canal indicates the presence of bifurcation in the main canal in the buccolingual direction.
* Professor & H.O.D.
** Associate Professor,
*** P.G. Student
Department of Conservative Dentistry& Endodontics, Guru Nanak Dev Dental College and Research Institute, Sunam (Punjab)
CASE REPORT
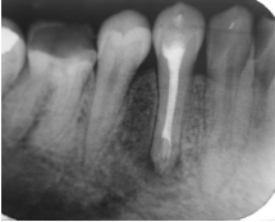
A 22 year old girl reported to the Department of Conservative Dentistry & Endodontics, Guru Nanak Dev Dental College, Sunam with complaint of pain and swelling in the mandibular right posterior region. Extra oral examination showed diffuse swelling on lower right side of the face, while intra oral examination revealed diffuse swelling obliterating the sulcus and presence of sinus in 44 region. The tooth was tender on percussion and exhibited grade 1 mobility. IOPA radiograph of 44 revealed a radiolucent area periapically, a large single canal upto the middle third of root, and suddenly bifurcating into two fine canals one mesially and one distally. (Figure 1)
 |
 |
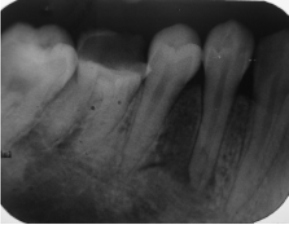
Vitality test showed that the tooth was non vital. Access was gained without giving any local anaesthesia. The orifice of canal was explored with no.15 K file. Once one canal was located, the file was left in the canal and another file number 10 K file was used to locate the other canal. The working length radiograph was taken (Figure 2) and the tooth was left open for drainage. Patient was advised to take antibiotics and warm saline rinses.
Patient was recalled after 2 days. Patient returned without pain and swelling. Biomechanical preparation was done and canals were prepared upto size 30. The canals were irrigated with saline and 0.2% chlorhexidiene. The canals were then dried with sterilized paper points, and calcium hydroxide dressing was given in the canals and the access was closed with Cavit. Patient was recalled after 3 weeks. When patient returned she was totally comfortable and sinus was healed. So Cavit was removed and canals were irrigated and dried. The root canals were then obturated with zinc oxide eugenol sealer and laterally condensed gutta percha. Both the canals were filled simultaneously. (Figure 3)
DISCUSSION
Brescia considered that morphology of first mandibular premolar was the most variable in the entire dentition. Vertucci (1978) reported that mandibular first premolar having type I canal in 70% cases, type II canal in 4% cases and type III in 1.5% cases while type IV canal present in 24.0% of the cases. In type IV canal, root canal bifurcated in the apical third region and thus showed two foramina.
Hence, it is recommended that clinicians should consider a thorough assessment of radiographs before treatment of mandibular premolars and have a true concept of the number of root(s) and canal(s). Special attention must be given to the preparation of a correct access cavity that is the key to finding all orifices and a successful treatment. The concept of mandibular premolars with one canal should not be considered as a rule.
References:-
1. Bellizzi, R. And Hartwell, G. : Evaluating the maxillary premolar with three canals for endodontic therapy. J.Endo: 7, 521-7, 1981.
2. Brescia, N.J., Applied Dental Anatomy, S.T.Louis, C.V.Mosby, pp.48,1961.
3. Bystrom, A., Claesson, R. And Sundqvist, G.: The antibacterial effect of camphorated phenol and calcium hydroxide in the treatment of infected root canals. Endodontics and dental Traumatology: 1, 170-5, 1985.
4. Stabholz, A., Zach, A. And Freidman, S.: Endodontic treatment of bifuracated mandibular premolars. Quint. Int.:4,301-302,1985.
5. Trope, M., Elfenbein, L.& Tronstad, L.: Mandibular premolars with more than one root canal in different race groups. J Endo.:12,343-345,1986.
6. Vertucci, F.J.: Root canal morphology of mandibular premolars. J.Am.Dent.Assoc.: 97,47-50, 1978. |