Introduction:
Increased demand for esthetics resulted in the evolution of ceramic brackets[1],[2]. Besides the high esthetic value ceramic brackets have poor fracture toughness[3],[4]. Enamel has little ability to absorb stress and is likely to be damaged during debonding of ceramic brackets[5]. Enamel fracture or the appearance of fracture lines during debonding is related to the high bond strength of ceramic brackets and seems to be associated with sudden impact loading [3],[6],[7],[8].
Various techniques for debonding ceramic brackets were developed[9],[10],[11]. However, an evaluation of effects of various debonding techniques on the enamel surface is required to gain knowledgeof their clinical success. Hence this study was undertaken with the aim to evaluate the enamel surface characteristics following debonding of ceramic brackets using different debonding techniques.
Materials & Methods:
Sixty extracted human maxillary premolar teeth which are free of caries, restorations and wasting disorderswere collected, cleaned using ultrasonic cleaner and stored in normal saline.
All the samples were examined for surface defects under stereomicroscope (SZX10 Olympus)with 10X magnification. Teeth with surface defects were eliminated and final sample of 60 teeth were mounted in the wax blocks (Figure 1) and prepared for the bonding procedure.
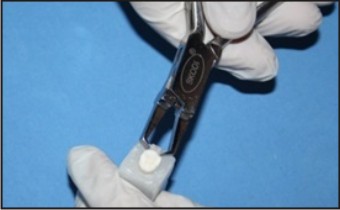 | Fig 1: Conventional Debonding.
 |
Bonding Procedure
1. Enamel surface was etched with 37% phosphoric acid (d-tech) for 30 seconds, rinsed thoroughly with water and dried with moisture free air until enamel had frosty appearance.
2. Primer (Transbond XT, 3M Unitek) was applied to the etched enamel surface in a thin film and photo polymerized for 10 seconds.
3. Adhesive (Transbond XT, 3M Unitek) was applied and the brackets were positioned properly on samples, excess flash was removed and polymerized for 20 seconds.
After proper bonding, the samples were randomly divided into 4 equal groups.
Group 1:
The first group of 15 teeth was debonded with conventional debonding plier (Skodi Orthodent) (Figure 1). The stainless steel blades of the plier were wedged at the bracket adhesive interface and a gentle squeezing action was applied until bond failure occurred.
Group 2:
In the second group brackets were debonded by application of heat using customized electrothermal debonding unit (25Watt soldering unit, Poze electronics , New Delhi) which was a 25Watt soldering rod that can produce a temperature of about 400 – 500 °c as measured using the thermocouple(Data Logger AI – 800 D, ACE Instruments, Hyderabad) (Figure 2). The tip of the unit was placed over the bracket for a period of 5 to 6 seconds for heat application and the heat generated was recorded with a digital meter attached to thermocouple. After application of heat for a brief period, the brackets were debonded with the conventionl debonding plier.
 | Fig 2: Electrothermal Debonding.
|
Group 3:
In this group TFI-1000, 25K Ultrasonic tip and the Cavitron Ultrasonic unit (Dentsply) were used to debond the brackets (Figure 3). The tip was placed at the adhesive bracket interface with the bevel of the scalar tip towards the bracket and was moved in a mesiodistal direction until a groove or "purchase point" approximately 0.5 mm in dimension was created in the composite between the bracket base and the enamel surface. A rocking motion was then applied to break the bond and facilitate bracket removal.
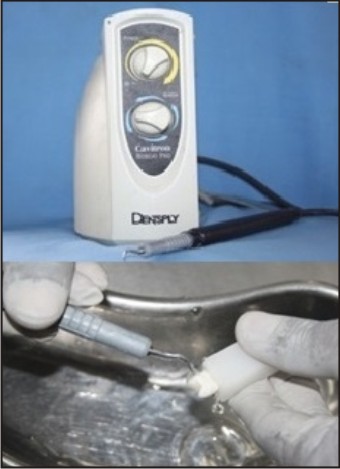 | Fig 3: Ultrasonic Debonding.
|
Group 4:
In the fourth group the teeth were placed in the peppermint oil (L-Menthol: 37-40%, Falcon Essential Oils, Banglore) for 5min followed by debonding the brackets using conventional plier (Figure 4).
 | Fig 4: Chemical Debonding.
|
After debonding, Adhesive Remnant Index (ARI) was scored using stereomicroscope at 10X magnification.
Score 1 – All the composite remained on the tooth
Score 2 – More than 90% of composite remained on the tooth
Score 3 – More than 10% but less than 90% of composite remained on tooth
Score 4 – Less than 10% of composite remained on the tooth surface
Score 5 – No composite remained on the enamel
A note was made on the site of bond failure (SF) during debonding as a part of scoring the remnant adhesive as follows.
Type 1: Ninety percent or greater of the bracket pad was exposed and 10% or less of the bonded enamel was free of composite resin.
Type 2: Less than 90% but more than 10% of the bracket pad was exposed or more than 10% but less than 90% of the bonded enamel surface was free of composite resin.
Type 3: Ten percent or less of the bracket base was exposed and 90% or more of the bonded enamel was free of composite resin.
Type 4: Fracture of the bracket during removal left a portion of the bracket still bonded to the enamel.
Type 5: A portion of the enamel was removed with the bracket base without loss of more than 10% of the composite resin from the bracket pad.
During the process of deboning the failure rate of the brackets (BF) was also recorded on a scale of 0 to 4, where 0 = no fracture, 1 = 1-wing fracture, 2 = 2-wing fracture, 3 = 3-wing fracture, and 4 = total fracture.
Following debonding, two teeth from each group having highest ARI scores were examined using scanning electron microscopic (SEM) (Hitachi, S - 3400N, Japan)to record the enamel surface details such as fractures, cracks or surface gouging.
Statistical Analysis:
Descriptive statistics were calculated individually for ARI, SF & BF in each group which included Mean and Standard Deviation.
One way ANOVA test followed by Tukey’s post hoc procedure was done for the comparison among the four groups. The data management was done in Statistical Package for Social Science, version 17(SPSS Inc., Chicago, Illinois, USA) and the ‘p’ value was set at 0.001 for all tests.
Results:
In the present study, enamel damage following debonding was assessed using ARI, site of bond failure and bracket failure indices. The enamel surface topographic details were evaluated under scanning electron microscope at 25X and 40X magnifications.
The results of the Adhesive Remnant Index, Bracket Failure and Site of bond Failure were shown in (Table 1). Mean ARI, BF, SF were calculated and compared among the study groups with ANOVA.
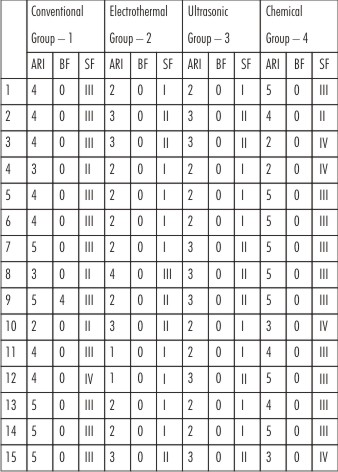 | Table 1 : Ari, Bf, Sf Scores In Various Debonding Techniques
|
(Table 2), shows the comparison of ARI among the four study groups. The results showed that Mean ARI was significantly different among the 4 study groups (p<0.001) with highest ARI scores of 4.07 ± 0.88 and 4.13 ± 1.13 for conventional and chemical debonding techniques respectively. The electrothermal and ultrasonic debonding techniques had scores of 2.27 ± 0.08 and 2.42 ± 0.52 respectively. Post-hoc analysis was done to evaluate inter-group comparisons. The Mean ARI was significantly more for group 1 than group 2 and 3. Similarly group 4 had higher mean ARI than group 2 and 3. No significant difference in the mean ARI was seen between group 1 and 4, group 2 and 3.
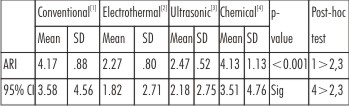 | Table 2 : Comparison Of Ari Scores Among The 4 Study Groups
|
(Table 3), shows the comparison of the Bracket Failure (BF). In Conventional debonding technique one sample was fractured completely including the bracket base and tie wings and two other samples showed minor bracket base fracture. No BF was recorded in other groups.
 | Table 3 : Comparison Of BF Scores Among The 4 Study Groups
|
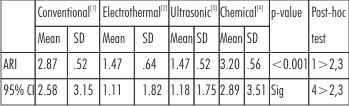
(Table 4), shows the comparison of site of bond failure among the four groups. The results showed that Mean SF was significantly different among the 4 study groups (p<0.001) with chemical debonding group having the highest mean score of 3.20 ± 0.56 followed by conventional debonding group with a mean score of 2.87 ± 0.52. Electrothermal and ultrasonic debonding groups had mean scores of 1.47 ± 0.64 and 1.47 ± 0.52 respectively. The Post-hoc Tukey’s test showed that the mean SF was significantly more for group 1 than group 2 and 3. Similarly group 4 had higher mean SF than group 2 and 3. No significant difference in the mean SF was seen between group 1 and 4, group 2 and 3.
 | Table 4: Comparison Of SF Scores Among The 4 Study Groups
|
SEM examination of the conventionally debonded samples showed enamel cracks and complete loss of perikymata at 40X magnification. The samples in electrothermal debonding group showed remnants of the adhesive, disturbance in the perikymatous structure and few areas of enamel surface loss. Ultrasonically debonded samples had gouging of the surface enamel where the scalar tip was placed for the purpose of debonding. Enamel surface of the chemically debonded samples showed remnants of adhesive with ill defined perikymata.
Discussion:
It is an important consideration that the entire bracket be removed in full while debonding because any sort of fracture of bracket will result in patient discomfort, increased chair side time and the possibility of swallowing or aspirating a bracket fragment[12]. Different manufacturers have come forward with a variety of debonding techniques, claiming the safety of ceramic bracket debonding.
The ARI scoring was based on the criteria followed by Samir Bishara et al[13] in their study in 1995 which was later adopted by Marc.E.Olsen et al[14] and Lina.P.Theodorakopoulou et al[15].
Bracket failure during debonding was scored based on the criteria given by Pramod.K.Sinha et al[16]. And for determination of the location of bond failure the samples were classified into 5 types based on the scoring criteria given by Hyer.K.E[17] which was later followed by Joseph M. Bordeaux et al[18] in 1994 and Vittorio Cacciafesta et al[19] in 1998.
Conventional Debonding Technique
The delamination technique as advocated by Swartz ML[5], Samir E. Bishara et al[20] and Pramod K.Sinha et al[16] was used. The pliers work either through the deformation of the bracket, breaking the bond at the bracket adhesive interface or by stressing the adhesive to its ultimate strength causing a cohesive failure within the composite resin and sometimes the failure may occur at the adhesive–enamel interface as stated by Samir Bishara et al[21].
About 46.6 % of the brackets had ARI score of 4 and 33.3% had a score of 5 which is in agreement with the ARI scores reported by Bishara et al[20],[21]. Bracket failure rate was very minimal however Bishara et al[20] in 1990 registered a bracket failure rate upto 35%. About 90% samples had bond failure at the enamel adhesive interface with more chance of enamel damage.
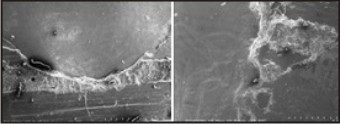
When viewed under Scanning electron microscope at 25X and 40X magnification (Figure 5), the enamel surface of the conventionally debonded samples showed enamel cracks and loss of surface enamel. These findings were similar to those of Keith V.Krell et al[10], where the conventional debonding plier (Unitek) was used. However, Samir E.Bishara et al[20] (1990) showed no evidence of enamel damage though the site of bond failure was at adhesive enamel interface.
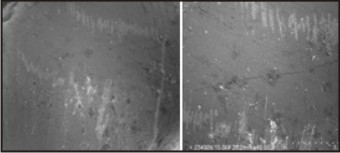 | Fig 5: Sem Images Of Conventionally Debonded Sample At 20 & 40 X Magnification.
|
Electrothermal debonding technique (EDT)
Several authors Margurite Crooks et al[22], Thomas.B.Redd et al[6], Joseph.S.Dogvan et al[23], Edwin M.M.Brouns et al[24] etc., in the past used a variety of electrothermal debonding equipments. However, at present no commercially produced electrothermal debonding equipment is available. Arthur L.Wool[25] used a wood burning pen that was capable of producing 400º - 500ºC of heat. Similar to Arthur L. Wool a 25 watt soldering rod was used for electrothermal debonding.
Samir E. Bishara et al[20] showed that the EDT gave an ARI score of 1 in about 85% of the samples. Marguerite Crooks et al[22] in 1997 showed similar findings. In the current study, about 60% of the samples have complete adhesive remained on enamel surface. There were no incidences of bracket failure, similar to S.Dogvan et al[23]. The site of bond failure ranged between type I to III with 60% of samples having type I bond failure, indicating less chance of enamel damage[26].
The SEM images of the electrothermally debonded samples (Figure 6) showed minor patches of enamel loss in the composite denuded regions. Kearns et al[27] observed no gross enamel fractures following SEM examination of debonded enamel. This clearly indicates that in the electrothermal debonding technique with most samples having type I bond failure, the damage of the enamel would be minimal.
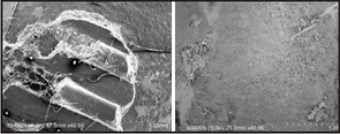 | Fig 6: Sem Images Of Electrothermally Debonded Sample At 20 & 40 X Magnification.
|
Ultrasonic debonding techniques
About 53% of the samples debonded ultrasonically had ARI score 2 and the rest had score 3. The Site of bond failure was of type 1 and type 2, indicating bracket failure at the adhesive-bracket interface or within the adhesive, similar to the findings of Daniel.B.Boyers et al[28]. With ultrasonic technique, the likelihood of enamel damage and bracket failure was minimal because of relatively low debonding force levels. Study by Daniel.B.Boyers et al[28] showed that the force required to remove ceramic brackets with ultrasonic tip was 0.28MPa. No bracket failure was noted which was similar to the earlier studies by Samir Bishara et al[20] and Daniel.B.Boyers et al[28].
SEM examination (Figures 7) showed minimal loss of surface architecture with distinctly seen perikymata. However enamel gouging was observed at the margins of the adhesive where ultrasonic tip was used. These findings were similar to Keith Krell et al[10].
 | Fig 7: Sem Images Of Ultrasonically Debonded Sample At 20 & 40 X Magnification.
|
Ultrasonic debonding was associated with excessive wear of the expensive tip and the need for a water spray to reduce the heat buildup which could cause pulpal damage[20],[29]. It also had a distinct drawback on the time consumed for debonding which was in sharp contrast to other debonding techniques as described by Bishara et al[22].
Chemical Debonding Technique
Chemical debonding of the ceramic brackets showed that 60% of the samples have complete adhesive removed from the enamel surface. Site of bond failure for most of the samples was type 3 and 4, indicating that the bond failure was at the enamel adhesive interface, which was similar to the findings of Larmour et al[30].
Waldron and Caustron[11] (1991) suggested that peppermint oil could have an effect when applied for very short periods (1–2 minutes) but work by Larmour and Chadwick[31] (1995) found no appreciable composite softening effect at such short periods. However Larmour et al[30] in 1998 showed that with both 5 minute and 1 hour placement of the bonded ceramic brackets in peppermint oil to facilitate ceramic bracket debonding did increased the incidence of bond failure at the enamel/resin interface. The enamel surface topography (Figure 8) showed no major enamel damage (cracks, gouging) except for mild loss of surface perikymata. This suggests that though in the chemically debonding technique, bond failure occurred at the enamel-adhesive interface the likelihood of the enamel damage was minimal, which might be due to the softening effect of the peppermint oil on the adhesive decreasing the bond strength.
Limitations of the study:
1) Conventional debonding plier used in the study showed highest incidence of enamel damage. However several manufacturers have come out with a variety debonding pliers, which were claimed to cause less enamel damage.
2) The temperature produced by the electrothermal unit might raise the intrapulpal temperature leading to pulpal damage which needs to be evaluated.
3) The debonding forces which might be different among the study groups were not measured.
The conclusions of the present study are as follows:
1) Conventional and chemical debonding techniques with high ARI scores had most common site of bond failure at enamel-adhesive interface which is detrimental to enamel surface. However SEM showed minimal enamel damage with chemical debonding.
2) Bracket failure rate was negligible.
3) Conventional debonding showed greater enamel damage than other methods.
4) Electrothermal and ultrasonic debonding techniques had bond failures at adhesive-bracket interface with minimal enamel damage.
5) Chemical debonding technique, with minimal enamel damage would be a better technique for debonding ceramic brackets.
References:
1. Russell. J. S. Current Products and Practice Aesthetic Orthodontic Brackets. Journal of Orthodontics, Vol. 32, 2005, 146–163.
2. Buonocore M. A simple method of increasing the adhesion of acrylic filling material to enamel surface. J Dent Res. 1955;34(6):849-53.
3. William A. Brantley, Theodore Elliades. Orthodontic materials scientific and clinical aspects. 1st ed.Thieme publications, Newyork, 2001.
4. Bishara S.E, Oslen M.E, Von Wald.L. Evaluation of debonding characteristics of a new collapsible ceramic bracket. Am J Orthod Dentofacial Orthop.1997;112:552-559.
5. Swartz M.L. Ceramic Brackets. J Clin Orthod. 1988;22:82-88.
6. Redd TB, Shivapuja PK. Debonding ceramic brackets: effects on enamel. J Clin Orthod 1991; 25: 475–81.
7. Scott GE Jr. Fracture toughness and surface cracks – the key to understanding of ceramic brackets. Angle Orthod. 1988;59:5-8.
8. Jeiroudi MT. Enamel fracture caused by ceramic brackets. Am J Orthod Dentofac Orthop 1991; 99: 97-99.
9. John J. Sheridan, Glenn Brawley, Joe Hastings.Electrothermal debracketing: An Invitro study, Am J Orthod Dentofacial Orthop. 1986;89:21-27
10. Keith V. Krell,Orthodontic bracket removal using conventional and ultrasonic debonding techniques, enamel loss, and time requirements.Am J Orthod Dentofac Orthop 1993;103:258-66.
11. Waldron, M. and Causton, B. E. A study of the fracture toughness of a light cured adhesive, Journal of Dental Research, 70, 696-702.
12. Winchester LJ. Methods of debonding ceramic brackets. Br J Orthod 1992; 19: 233–237.
13. Bishara.S.E, Fonseca.J.M, Boyers.D.B. The use of debonding pliers in the removal of ceramic brackets. Force levels and enamel cracks. Am J Orthod Dentofac Orthop. 1995;108:242-248.
14. Olsen.M.E, Bishara.S.E, Boyer.D.B, Jakobsen.J.R. Effect of varying etching times on bond strength of ceramic brackets. Am J Orthod Dentofac Orthop 1996;109:403-409.
15. Theodorakopoulou.L.P, Sadowsky.P.L, Jacobson.A, Lacefield.W. Evaluation of the debonding characteristics of 2 ceramic brackets: An invitro study. Am J Orthod Dentofac Orthop 2004;125:329-336.
16. Sinha.P.K, Nanda.R.S. Effect of different bonding and debonding techniques on debonding ceramic orthodontic brackets. Am J Orthod Dentofac Orthop.1997;112:132-137.
17. Hyer KE. An in vitro study of shear and tensile bond strengths comparing mechanically and chemically bonded ceramic brackets with three bonding agents. [Masters thesis]. Iowa City: University of Iowa, 1989.
18. Joseph M. Bordeaux, Robert N. Moore, Michael D. Bagby. Comparative evaluation of ceramic bracket base designs. Am J Orthod Dentofac Orthop 1994;105:552-560.
19. Vittorio Cacciafesta, Maria Francesca, Brite Melsen, Andrea Scribante. A 12 month clinical study of bond failures of recycled versus new stainless steel orthodontic brackets. European Journal of Orthodontics.2004;26:449-454.
20. Bishara S.E, Timothy S. Trulove.Comparisons of different debonding techniques for ceramic brackets: An in vitro study. Am J Orthod Dentofac Orthop 1990;98:145-53.
21. Bishara.S.E & Ferh.D.E. Comparision of the effectiveness of pliers with narrow and wide blades in debonding ceramic brackets. Am J Orthod Dentofac Orthop. 1993;103:253-257.
22. Marguerite Crooks, James Hood. Thermal debonding of ceramic brackets: An in vitro study. Am J Orthod Dentofac Orthop. 1997;111 :163 – 172.
23. Joseph S. Dovgan, Richard E. Walton, Samir E. Bishara. Electrothermal debracketing: Patient acceptance and effects on the dental pulp.Am J Orthod Dentofac Orhop 1995;108:249-55.
24. Edwin. M.M. Brouns, Peter M. Schopf, Bogdan Kocjancic. Electrothermal debonding of ceramic brackets: An invitro study. European Journal of Orthodontics. 1993;15:115-123.
25. Arthur L. Wool. A better debonding procedure. Am J Orthod Dentofac Orthop. 1992;102:1-4.
26. Todd Lee-Knight, Simon G. Wylie, Paul W. Major, Ken E. Glover and Michael Grace. Mechanical and electrothermal debonding: Effect on ceramic veneers and dental pulp. Am J Orthod Dentofac Orthop 1997;112:263-70.
27. Harry.O.Kearns, J.Andrew Sandham. W.Bryan.Jones, Lennart Lagerstrom. Electrothermal Debonding of Ceramic Brackets: An Ex Vivo Study. British Journal of Orthodontics 1979;24:237–242.
28. Daniel.B.Boyers, Geoffery Engelhardt, Samie E. Bishara. Debonding orthodontic ceramic brackets using ultrasonic instrumentation. Am J Orthod Dentofac Orthop 1995;108:262-266.
29. Ghafari.J. Problems associated with ceramic brackets suggest limiting use to selected teeth. Angle Orthod. 1992;2:145-152.
30. Larmour C.J, J.F.Mccabe, P.H.Gordon. An Ex vivo Investigation into the Effects of Chemical Solvents on the Debond Behaviour of Ceramic Orthodontic Brackets. British Journal of Orthodontics.1998;25:35-39.
31. Larmour, C. J. and Chadwick, R. G. Effects of a commercial orthodontic debonding agent upon the surface microhardness of two orthodontic bonding resins, Journal of Dentistry1995;23:37-4
|