Introduction
Conventional caries removal procedure involves the use of a drill, on a high speed handpiece to gain access to the carious lesions, and a low speed handpiece to remove carious dentine[1]. Many patients consider this process to be very unpleasant. Often this apprehension is due to pain/discomfort, local anaesthesia and the use of drilling during caries removal. In addition, the excessive noise of drill is also unpleasant. Dentin caries removal with the drill may be traumatic to the pulp due to pressure, thermal changes and vibration apart from equally removing infected and un-infected dentin, resulting in excessive loss of healthy tooth structure[2].
The techniques used in carious dentin removal have developed since GV Black, in 1893, initially proposed the principle of ‘Extension for Prevention’. These principles were constrained by the knowledge of the disease process and the restorative materials available at that time [3].
Systems for caries removal and cavity preparation have been under strong pressure for development towards minimal invasive procedures and increased patient comfort [1].
Due to the shortcomings of drill and local anaesthesia, there has been a growing interest in developing alternative techniques, which are more comfortable and preserve healthy dental tissues. These minimally invasive techniques are now possible due to the following developments: adhesive restorative materials, dispensing with mechanical retention during cavity preparation; restorative materials which release fluoride; biological understanding of the caries process and the teeth’s natural defense mechanism [2].
Latest concepts regarding the rationale of carious dentine removal are also beginning to questions the amounts of tissue that need to be excavated in order to successfully treat a carious lesion [3].
The subdivision of dentin caries into two layers of high and low levels of infectionand the fact that carious dentin with a low level of infection is halted under restorations have led to a new concept of treatment of dental caries. The aim became to remove only the layer with a high level of infection (infected dentin), preserving the layer with a low level of infection (affected dentin), which consists of tissues able to remineralize [2].
However in spite of a better understanding in the theory and rationale of caries treatment, the clinical approach has not changed. When removing dentin, the clinician may experience difficulties in diagnosing the borders of carious lesion, due to the apparent lack of objective clinical markers. Conventional visual and tactile criteria (Color and hardness of carious dentin) fail to be definite indicators of the depth or degree of carious dentin. Use of subjective criteria may result in different types and quantities of dentin removal, dependent on operator and not on nature of lesion itself. The histology and microbiology of a carious lesion has shown that carious lesion is not of homogenous nature. SEM and microhardness test methods revealed different layers of carious dentin. From a clinical perspective, the ability to discern between demineralized and mineralized dentin or between infected and affected dentin will allow the specification of carious treatment, forgetting the biologic sense. Also, conventional methods involving hand excavation and low speed drilling may remove softened but uninfected dentin and result in excessive loss of tooth structure [4].
An alternative was the introduction of new products for chemomechanical caries removal [5].
The Chemomechanical Systems:
a) History: The chemomechanical approach was initially introduced in 1972 in the form of original GK-101 solution. The GK-101 formula essentially consisted of N-monochloroglycine (NMG) and sodium hypochlorite. There were biochemical indications that the fibrillar organization of the collagen may be disrupted by GK-101. GK-101, however, proved too slow in caries removal rate and evolved into GK-101E, which was the basis for the United States Food and Drug Administration (FDA) acceptance (1984) of the commercial product Caridex™ (National Patent Medical Products Inc., New Jersey, USA). Caridex™, instead of N-monochloroglycine, contained N-monochloro-DL-2 amino butyric acid (NMAB), although the effects were based on much of same principles as those previously described for GK-101[6].
The Caridex system had certain clinical limitations including the efficacy of caries removal, the large volume of solution needed, short shelf life and the time taken[1]. The solution had to be heated in a reservoir and special pump was needed to supply the solution. The product’s expensive price and long working time made it unattractive and costly to the clinician. It was subsequently removed from the commercial market.
A new method for chemomechanical caries removal was then developed called Carisolv, (Mediteam) to meet the shortcomings of Caridex. The chemical composition was improved and significantly shortened the time necessary for complete caries removal, making this system an effective alternative to the rotary handpiece for the treatment of caries.
b) Carisolv: Carisolv consists of two carboxymethyl cellulose based gels in two vials: a red gel containing 0.1M aminoacids (l-glutamic acid, l-leucin acid and l- lysine acid), sodium chloride (NaCl), sodium hydroxide, erythrosine, and purified water at pH 11, and a clean 0.5% solution of NaOCl[4]. The mode of action of chemomechanical caries removal systems is by chlorination of partially degraded collagen and cleavage by oxidation of glysine residue, which results in collagen fibril disruption, making them more friable and easy to remove. The hard unaffected dentin is not removed. The advantage of Chemomechanical agents is that it selectively removes softened dentin and conserves the tooth structure, thereby lessening the chances of iatrogenic pulp exposure[7]. It is also highly probable that the gel has a mechanical lubricating action for the hand instruments which will also aid in removal of the softened tissue[3].
The gel is available in two different packages, Carisolv gel Multi mix (Figure 1) and Carisolv gel Single mix (Figure 2).
 | Figure 1: Carisolv Gel Multimix With Hand Instruments.
 |
 | Figure 2: Carisolv Gel Singlemix With Hand Instruments.
|
A, new, modified Carisolv gel has been developed in order to optimize the efficiency of its chemical caries dissolution[8]. It consists of an uncoloured gel and 0.95% Sodium hypochlorite solution. It is claimed to be 25% quicker than previous gel in caries removal and contains no potentially staining pigment, a problem identified with its erythrosine containing predecessor. This eliminated the concerns over esthetic compromise during use in anterior teeth. The selective and conservative features of Carisolv reduce the risk of direct pulpal exposure and allow continuing pulp vitality[9].
Indications: The clinical situations in which carisolv could be considered the preferred method of caries removal includes:
Where preservation of tooth structure is important;
The removal of root/cervical caries;
The management of coronal caries with cavitation;
Removal of caries at the margins of crown and bridge abutments;
The completion of tunnel preparations;
Where local anesthesia is contraindicated;
The care of caries in dentally anxious patients, notably needle phobics;
Management of primary carious lesions in deciduous teeth;
Atraumatic restorative technique procedures;
Caries management in patients with special needs[10];
Cases in which high predictability of caries removal is needed[4].
Manufacturer’s instruction: The gel does not affect healthy dentine or soft tissue. Nor does it affect enamel. Consequently carisolv should be used in combination with the drill or alternative techniques. Drilling could preferably be used whenever the cavity needs to be opened up, for adjustment of cavity periphery or whenever there are large amounts of caries and when the risk to affect healthy tissue is minimal.
1. Mix the two components of Carisolv® (NaOCl and amino acid solution) thoroughly according to the instructions included with the package. Put the required amount of gel into a suitable container.
2. Use a Carisolv® instrument (Figure 3, Figure 4) to pick up the gel and apply it to the carious dentine. Soak the caries generously.
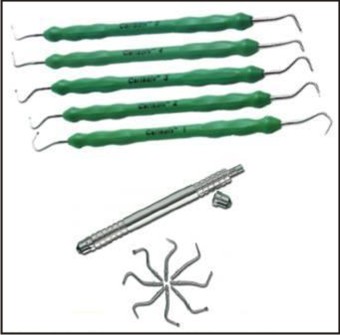 | Figure 3: Carisolv Hand Instruments.
|
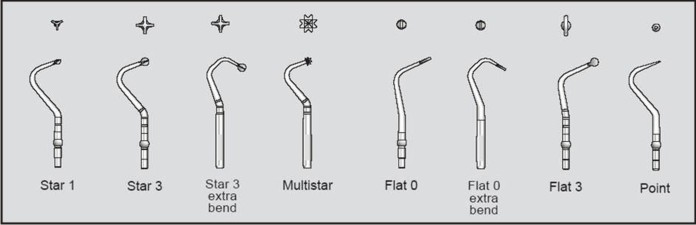 | Figure 4: Specially Designed Tips Of Carisolv Hand Instruments.
|
3. Wait for at least 30 seconds, for the chemical process to soften the caries.
4. Select a Carisolv® hand instrument to match the size, position and accessibility of the cavity. Scrape off the superficial softened carious dentine. The hand instrument with the multistar tip may facilitate the early penetration of the gel. Work carefully using scraping or rotating movements. Remove the softened carious dentine with the instrument. Avoid flushing or drying the cavity.
5. Keep the lesion soaked with gel and continue scraping. Repeat until the gel no longer turns cloudy and the surface feels hard using the instrument. Check extra carefully for caries at the dentinoenamel junction. If you are using a drill to adjust the periphery before filling, this can be done while the gel is still in the cavity.
6. When the cavity feels free from caries, remove the gel and wipe the cavity with a moistened cotton pellet or rinse it with lukewarm water, inspect and check it with a sharp probe. If the cavity is not free from caries, apply new gel and continue scraping.
Note: when the cavity is dried with air, the treated surface looks frosted and not shiny, as it does after excavation using a drill.
7. If necessary the periphery of the cavity should be adjusted using hand instruments or the drill. Restore the tooth with a suitable filling material according to the manufacturer’s instructions for use.
Note: Once the gel has been mixed, its caries softeningability will begin to decline after about 30 minutes.Any gel that is left over should be destroyed in accordancewith local regulations.
Storage: An opened package can be kept at room temperature during working hours. At all other times, it should be kept in a refrigerator. An opened package can be kept up to one month, for subsequent use.
Advantages:
Well documented and researched
Minimally-invasive, selective and precise
Minimizes the need for the drill and anesthetics and enhances patient comfort
Makes it possible to avoid drilling close to the pulp
Carisolv® instruments with sharp yet blunt cutting angles help to protect healthy tissue[11].
c) Papacarie: Despite its effectiveness, carisolv was not a blockbuster mainly because it required, 1) Extensive training and registration of professionals and 2) customized instruments which increased the cost of the solution. As a result, few people had access to the carisolv solution.
In 2003, a research project in Brazil led to the development of a new formula to universalize the use of Chemomechanical method for caries removal and promote its use in public health. The new formula was commercially known as Papacarie (Figure 5). It is basically comprised of papain, chloramines, toluidine blue, salts, thickening vehicle, which together are responsible for papacarie’s bactericidal, bacteriostatic and anti inflammatory characteristics. Papacarie is a national product; patented, registered and approved by ANVISA in Brazil[12].
Papain, a proteolytic enzyme, interacts with the partially degraded collagen of caries causing a further softening of the tissue. This proteolytic action occurs only in the necrotic tissue, because healthy tissue contains alpha-1-antitrypsin, an antiprotease that prevents the action of proteolytic enzymes. Thus, the non-necrotic dentin, with the possibility of regeneration, is preserved by the product. It is especially recommend to not cut the dentin, but to scrape it as papain only interacts with the degraded collagen and a cutting procedure can remove beyond what is necessary.
Chloramine, acts to promote the chlorination of collagen in the carious dentin, acting only in the portion of necrotic tissue, preserving healthy tissue. Thus, the composition of the product is aimed at synergistic action of papain and chloramine. This helps in the softening of necrotic portion of the decayed tissue, facilitating its removal, without cutting the structure and preserving the healthy dentin, in which the product does not act.
Toluidine blue,Initially, the malachite green was used as colouring agent, however, after a few studies toluidine blue was found highly effective against Streptococcus mutans. It is a photosensitive pigment that fixes into thebacterial membrane.
 | Figure 5: Papacarie.
|
There is no need to use any particular tool. The softened dentin is removed by scraping with a curette or any instruments with sharp yet blunt cutting angles. Hence, only the softened dentin and the soft gels are removed and sound dentin is preserved, without being cut by the instrument. It is highly selective and does not remove hard un-infected dentin. The product does not have adhesive characteristics and is fully washable in water without leaving residues that may interfere with the restoration of the tooth[13].
Instructions for Use:
1. Preparation for Use: Access to the carious dentin is obtained by removing the enamel with a high speed drills. Rubber dam can be used, if necessary. Remove the protective cap from the syringe and remove the desired amount of product, then pull the plunger back, wipe the tip with a paper towel and place the protective cover.
2. For the removal of carious dentin, fill the cavity with Papacárie.
3. Wait for atleast 30 seconds for acute caries and 40 to 60 seconds for chronic caries. This duration is required to allow for chemical softening of the caries. There is bubbling action seen.
4. The softened dentin should be removed with a suitable instrument like spoon excavator.
5. The gel should be reused as many times as necessary until there is no more presence of soft dentin.
6. There is no need for washing or drying the cavity between the applications of the gel.
7. When the gel remains with clear and unchanged color, it indicates that there are no more softened caries left.
8. An explorer with a rounded tip should be used to confirm if the cavity is free of infected tissue. If no caries are remaining, then remove the gel with a cotton ball soaked in water and fill the cavity with a suitable material.
Storage: Papacárie should be used at room temperature and need not necessarily be stored under refrigeration[13].
Advantages of papain gel
(1) Papacarie is a biocompatible gel with antibacterial properties that eliminates the need for anesthesia, removes only the compromised tissue, and preserves the healthy tissue better.
(2) The formation of a smear layer is not observed after using the gel.
(3) The gel combines an atraumatic treatment with antibacterial properties without affecting healthy tissue and causing pain[14].
Conclusion
The chemomechanical caries removing agents facilitates delivery of atraumatic and pleasant treatment while removing least amount of tooth structure without leaving any infected dentin. These agents can be used as a diagnostic tool in demarcating the borders of the lesions. This in turn helps in preventing any forceful and inadvertent pushing of carious debris and hence any spread of infection in to the pulp space, which can occur if caries are removed by conventional drill or hand excavation. Hence these agents would allow for conservative treatment procedures that would maintain the vitality of the pulp.
Both carisolv and papacarie are well researched and are clinically effective chemomechanical caries removing gels which are harmless to the healthy tissues. Hence, these are important agents of ‘Minimal Intervention Dentistry’ and they holdexcellent promise in future dental practice.
References
1. Ericson D, Zimmerman M, Raber H, Götrick B, Bornstein R, Thorell J. Clinical evaluation of efficacy and safety of a new method for chemo-mechanical removal of caries.Caries Res 1999 May-Jun; 33(3): 171-7.
2. Nadanovsky P, Cohen Carneiro F, Souza de Mello F. Removal of caries using only hand instruments: A comparison of mechanical and chemo-mechanical Carisolv methods. Caries Res 2001 Sep-Oct; 35(5): 384-9
3. Banerjee A, Watson TF, Kidd EA. Dentine caries excavation: a review of current clinical techniques. Br Dent J 2000 May 13; 188(9): 476-82.
4. Ziskind D, Kupietzky A, Beyth N. First choice treatment alternative for caries removal using the chemomechanical method. Quintessence Int 2005 Jan; 36(1): 9-14
5. Erhardt MC, Amaral CM, de Castro AK, Ambrosano GM, Pimenta LA. Invitro influence of Carisolv on shear bond strength of dentin bonding agents. Quintessence Int 2004 Nov-Dec; 35(10): 801-7.
6. Maragakis GM, Hahn P, Hellwig E. Chemomechanical caries removal: a comprehensive review of the literature. Int Dent J 2001 Aug; 51(4): 291-9.
7. Pai VS, Nadig RR, Jagadeesh T, Usha G, Karthik J, Sridhara K. Chemical analysis of dentin surfaces after Carisolv treatment. J Conserv Dent 2009; 12: 118-122.
8. Fure S, Lingström P. Evaluation of the chemomechanical removal of dentine caries invivo with a new modified Carisolv gel. Clin Oral Investig 2004 Sep; 8(3): 139-44.
9. Dammaschk T, Stratmann U, Mokrys K, Kaup M, Ott KH. Histocytological evaluation of the reaction of rat pulp tissue to Carisolv. J Dent 2001 May; 29(4): 283-90.
10. Morrow LA, Hassall DC, Watts DC, Wilson NH. A chemomechanical method for caries removal. Dent Update 2000 Oct; 27(8): 398-401.
11. Clinical Manual. August 25, 2010. Available at http:// www. mediteam. com / index.php ? option = com_content & task = view & id = 15 & Itemid = 17. Accessed April 14, 2012.
12. Bussadori SK, Castro LC, Galvão AC. Papain gel: a new chemo-mechanical caries removal agent. J Clin Pediatr Dent. 2005; 30(2):115-9.
13. Papacárie DUO Pediatric Dentistry and Prevention. Accessed April 14, 2012.
14. Ganesh M, Parikh D. Chemomechanical caries removal (CMCR) agents: Review and clinical application in primary teeth. Journal of Dentistry and Oral Hygiene 2011 Mar; 3(3): 34-45. Available from http://www.academicjournals.org/JDOH. Accessed April 14, 2012.PAPACÁRIE
|