Introduction
A captivating smile can surely be a booster to the self-confidence of individuals. Presently, dental professionals can use a variety of materials&techniques for smile enhancements ranging from orthodontic therapy to composite bonding, crowns & veneers. However, all the choices available for conservative cosmetic restorations should have but one common goal - a marriage between esthetics and durability[1]. The ultimate success of a cosmetic case and patient satisfaction is accomplished with the proper union of restorative materials, well-planned tooth preparation, dependable bonding, biologically acceptable soft-tissue treatment, and accurate communication between the patient, dentist, and laboratory[2].
Porcelain laminate veneers (PLVs)have been placed for more than 20 years meeting the esthetic desires of most patients[3]. When it comes to restoring the mouth with porcelain for this expressed purpose, the PLVs are one of the most conservative and aesthetic techniques that we can apply. The longevity of the veneers is quite long and durable especially if the right indications are chosen and the correct techniques are applied[4].
One of the major indications of utilizing PLV is space management. It becomes more of a challenge if the teeth are spaced or the teeth are not aligned properly on the dental arch, such as crowding. A preparation model and guide are very helpful to the dental practitioner in this regard, as they allow him or her to visualize the amount of tooth reduction necessary to achieve the desired aesthetic result.
Too often, more tooth structure is removed than is necessary in preparation of misaligned teeth, which can result in an increase in tooth sensitivity or a less retentive bond as all the enamel is removed unnecessarily. The more conservative the tooth preparations the greater the life expectancy of the veneer restorations.This presentation describes a patient who had rejected orthodontic therapy but continued to seek an improved cosmetic result. Porcelain veneers and crowns were an appropriate alternative in this case.
Case Report
A 21 yr old female patient reported to us with a profound spacing in the maxillary anteriors. Pressed with the demand s of a pending engagement, the young patient wanted an esthetic makeover within a short period of time. Clinical examination revealed a relatively healthy dentition with adequate oral hygiene. However, gaps were present between 11, 12, 13,21, 22 & 23 in the upper jaw (Fig. 1). Tooth number 22 was grossly out & far too labially placed with respect to others in the arch (Fig. 2a). Also a large gap existed between 41&42 & a mild space between 31&32 in the lower jaw (Fig. 2b).The initial diagnostic evaluation consisted of thorough extra- and intraoral examinations, temporomandibular joint and muscle evaluation, a series of digital photographs, and the mounting of study casts in centric relation. No joint or muscle tenderness was noted. On the basis of above examinations, the patient was presented with the two alternative treatment plans viz. (1). Orthodontic correction of her gaps or (2). Closure of her spaces with minimally invasive PLVs, crowns & composite bonding. Orthodontic correction necessitated a time frame of at least one & a half years but as time constraint was a major issue, upon consultation with the patient, it was decided to take up a the minimally invasive approach to smile design.
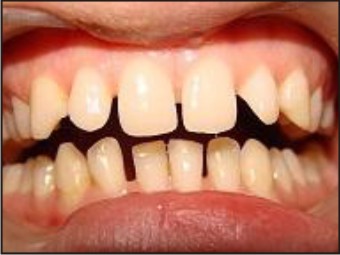 | Fig. 1 : Preoperative View Of Anterior Spacing
 |
 | Fig. 2a : 22 In Labioversion
|
 | Fig. 2b : View Of Spaces On The Right Side
|
To begin with a direct composite mock-up of the maxillary anteriors was performed to check tooth proportions, phonetics, esthetics, and act as a color preview & and was shown to the patient as the first “preview” of desired treatment. Thereafter a diagnostic wax up was carried out to further ascertain & gauge the final treatment outcome (Fig. 3).
 | Fig. 3 : Diagnostic Waxup
|
On the basis of both these procedures it was decided that IPS emax porcelain laminate veneers(Ivoclar vivadent) would be placed on five maxillary anteriors 11,12.13,21,23,but for 22 which necessitated greater removal of facial enamel to preserve the arch form, making it a candidate for a full coverage crown. Further, an emax full coverage crown on 42 & a composite buildup on the distal of 41would be needed to close this gap. Also, a composite buildup on the distal of 31 & mesial of 32in the mandibular arch to eliminate the gaps between the adjacent teeth was planned. Composite buildups were planned on both the adjacent teeth so as to avoid making them look wider mesiodistally. All the five upper anteriors needed to be prepared minimally to achieve the desired results. Reduction commenced with the establishment of arch form. Initially 0.3-mm depth cuts were made on all of the teeth, and then a medium, round-ended, diamond bur was used to remove a uniform thickness of facial enamel by joining the depth-cut grooves. As closure of gaps was the objective, the finish line was taken more lingually toward the lingual transitional line angle so that the contour of the porcelain can be started from the lingual and be built up to properly close the interproximal space. This aids in concealing the visibility of the interproximal margins of the veneer as well. A light chamfer finish line of 0.3 mm gingivally and interproximally was achieved so that ceramist could clearly see where to terminate the restoration. The facial incisal line angle was rounded slightly to minimize any stress concentration in the ceramic. By preparing the minimal amount of tooth structure, significant amount of enamel was conserved. However, tooth number 22 & 42 were prepared for full coverage restorations with a reduction of 1.5 mm on all the surfaces & a butt joint of 1mm at the cervical finish line.
Impressions were then made & face-bow transfer and a bite registration perfomed with an interpupillary recording stick. These records were then used to orient the maxillary model on the articulator(Stratos300-Ivoclar Vivadent) they helped in aligning the incisal edges & preventing canting while the definitive restorations were fabricated.
The shade of the prepared teeth was then recorded and communicated to the laboratory technician alongwith the preoperative digital photographs of the patient. Instructions were given to the technician to introduce a slight increase in hue in the cervical region, with subtle incisal translucency to be blended into the final restoration so as to achieve a polychromatic effect that would complement the existing dentition.
When returned from the laboratory, the restorations were evaluated for marginal integrity on the trimmed working dies and solid models. (Fig. 4a, 4b). The restorations were first tried in with water to verify marginal fit and then with try-in gel (Variolink Veneer, Ivoclar Vivadent) to evaluate shade and aesthetics. The veneers & crowns were tried out one by one in order to check the margin fit accurately, and then together, to see their overall integration with each other, with the lips and finally, the face.The dual-curing, highly esthetic luting composite Variolink Veneer, (Ivoclar Vivadent) which distinguishes shades by value was used to bond the veneers into place.Lithium disilicate (LS2) restorations were etched with IPS Ceramic etching gel for 20 seconds to generate a retentive bonding surfaces on all-ceramic restorations. It enhances the bonding effect between the luting composite and the ceramic bonding surface.The prepared teeth were pumiced and etched with phosphoric acid.Once the teeth and the inside of the veneers were surface treated they were now bonded two by two. The restorations were seated together using the rapid cementation technique .We started, the bonding with the centrals, proceeding with the lateral, canine on one side and then the lateral & canine on the other side. The soft tissues were handled very gently. After placing the veneer on the tooth and once it was completely seated. First, light curing was done for the excess flash around the gingiva for only 1 or 2 seconds. This did not fully polymerize the luting resin but brought it to a jellylike consistency that was very easily cleaned with an explorer dipped in an adhesive liquid. Then, we went in between the veneers with a dental floss to cleanse the interproximal contacts. Once everything was cleaned, luting resin was completely polymerized. After the bonding procedure a #12 blade was used to cleanse the undetected leftover composite on the margins and then the margins were polished with a rubber cup. Thereafter, the lower emax crown was bonded in the similar fashion on 42.Following this composite bonding was performed on distal of 41, distal of 31 & mesial of 32 in order to eliminate the respective gaps. The patient returned to the office one week later to permit a final examination of aesthetics, phonetics, and occlusion. She was satisfied with the aesthetic enhancement achieved through this predictable restorative procedure (Fig. 5).
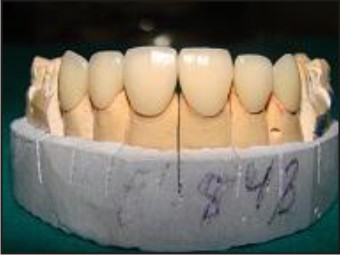 | Fig. 4a : Maxillary Model With Definitive Restorations Labial View
|
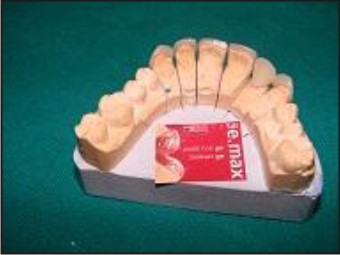 | Fig. 4b : Maxillary Model With Definitive Restorations Palatal View
|
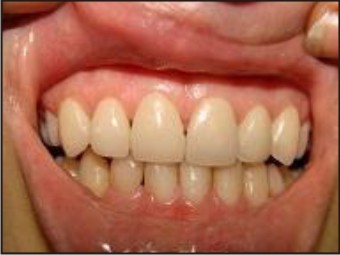 | Fig. 5 : Postoperative View With Veneers In Place
|
Discussion
Porcelain laminate veneers, by nature are a conservative treatment modality that provides excellent potential for aesthetic enhancement when their indications are respected. When restoring the teeth with PLVs, there are two problems which come along when teeth are not aligned properly on the dental arch: a) visualizing the aesthetic outcome, b) tooth preparation. Because the patient must be pleased with the treatment, a predictable approach should be used to enroll them in the restorative process as soon as feasible. During consultation, it is of utmost importance to discuss the patient’s desires, concerns, and limitations, and to discern whether they are emotional, financial, or for another reason. From the outset, it is critical that the dentist be able to articulate and create a vision of the anticipated aesthetics for the patient[5]. To avoid any miscommunication and ensure a successful result, there are certain options the dentist has at his or her disposal to demonstrate the appearance of the anticipated outcome prior to treatment. Computer imaging or a composite mock-up has shown to be helpful in demonstrating the appearance of longer teeth or a fuller smile[6].
Once PLV is the choice of restoration, preservation of sound tooth structure must remain a goal throughout the tooth preparation[7]. The dentin-enamel junction (DEJ) is very important in the structural strength of the tooth. The explanation lies in the most fascinating feature inherent to the natural tooth - a complex fusion at the DEJ, which can be regarded as a fiber reinforced bond[8]. Because when we limit our preparations on enamel, the tooth will not flex and it will stay as rigid as a tooth can be[9]. Even if our preparation line passes through the DEJ margin and enters into dentin, it won’t create a major problem for minor invasions. However, if we end up finishing our preparation on large amounts of dentin, we may end up with other kind of problems. Over preparing the rotated or aggressive preparation of protrusively placed teeth will cause us to end up in the dentin structure which will lower our bonding values as well as causing the flexing of the tooth structure[10]. And when the tooth starts flexing the luting resin at the margin will start peeling off slowly& we end up with some micro-leakage or delamination., In order to minimize those effects and problems, we have to be very precise and careful about case selection and tooth preparation[11] .The ideal cases in which we would want to place the veneers are when the teeth are aligned perfectly on the dental arch and maintaining their original facial volumes which means that the facial structures of the teeth isn’t worn as it happens by aging. In other words, we exactly need to remove the tooth structure equivalent to the thickness of the veneer that we will be placing on the tooth itself. Ideally, this philosophy also entails the clinician’s preparation of as few teeth as possible to obtain the desired aesthetics.
One decision that always needs to be considered is whether adjunctive orthodontics should be completed to place the teeth in the ideal position so that there is minimal or no reduction for bonded porcelain. Ideally, if the teeth require bonded porcelain anyway for reasons of form correction, closure of gaps, color alteration, or replacement of failed restorations and the amount of healthy tooth structure removal will be similar even if orthodontics is done, then bonded porcelain without adjunctive orthodontics should be accomplished. But if orthodontics significantly reduces the need for healthy tooth structure removal, specifically, if the preparation has to cross the dentinoenamel junction, then orthodontics should be first completed[12].
Conclusion
Choosing the perfect treatment plan for a patient with anterior gaps is a highly subjective matter & requires a multifactorial approach. Apart from all other aspects the time frame required to achieve the same is of paramount importance. The use of the mock ups, wax ups and silicone index allows us to select the appropriate plan & material required for the best aesthetic, phonetic and functional outcome.PLVs have been shown to be one of the most conservative & aesthetic restorations in this regard which can provide the desired results with minimum invasion on the recipient tooth & within a short period of time.
References
1. Tipton PA. Aesthetic tooth alignment using etched porcelain restorations. Pract Proced Aesthet Dent. 2001; 13(7):551-555.
2. Dumfahrt H. Porcelain laminate veneers. A retrospective evaluation after 1 to 10 years of service: Part 1 – Clinical procedure. Int J Prosthodont. 1999; 12(6):505-513
3. Swift EJ Jr, Friedman MJ. Critical appraisal: porcelain veneer outcomes, part II. J Esthet Restor Dent. 2006; 18(2):110-113
4. Horn HR. Porcelain laminate veneers bonded to etched enamel. Dent Clin North Am 1983; 27:671-684.
5 Smallwood T. Fabricating the undetectable smile: Choose natural over artificial. J Cosmetic Dent 2006; 22(1):94-103.
6. Mizrahi B. Visualization before finalization: A predictable procedure for porcelain laminate veneers. Pract Proced Aesthet Dent 2005; 17(8):513-518.2L
7. Milnar FJ. Mastering minimal intervention and discretionary aesthetic procedures when placing direct composites. Pract ProcedAesthet Dent 2005; 17(6):428-432.
8. Lin CP, Douglas WH, Erlandsen SL. Scanning electron microscopy of type I collagen at the dentin-enamel junction of human teeth. J Histochem Cytochem1993; 41:381-388.
9. Magne P. Douglas WH. Porcelain veneers: Dentin bonding optimization and biomimetic recovery of the crown. Int J Prosthodont 1999; 12:111-121.
10. Noack MJ, Roulet J-F. Rasterelelektronenmikroskopische Beurteilung der Atzwirkung verschiedener Atzgele auf Schmelz. Dtsch Zahnarztl Z 1987; 42:953-959) (Van Meerbeek B, Peumans M, Gladys S, et al.Three-year clinical effectiveness of four total-etch dentinal adhesive systems in cervical lesions. Quint Int1996; 27:775-784)(Van Meerbeek B, Perdigao J,Lambrechts P, et al. The clinical performance of adhesives.J Dent 1998;26:1-20.
11. Besler UC, Magne P, Magne M. Ceramic laminate veneers: Continious evolution of indications. J Esthet Dent 1997; 9:197-207
12. Edward A. McLaren .Porcelain Veneer Preparations:To Prep or Not to Prep.Inside dentistry 2006(5):76-79
|