Introduction
For root canal treatment to be successful, it is necessary to locate all root canals, debride them thoroughly and seal them completely with an inert root filling material. Unfilled canals remain a nidus for infection and can compromise treatment outcome. An awareness and understanding of the presence of unusual root canal morphology can thus contribute to the successful outcome of root canal treatment. The majority of first molars are two-rooted with two mesial and one distal canal[1],[2]. Ghoddusi[3] reported the presence of 4 distal canals in mandibular first molar. A number of anatomical variations have been described in the mandibular first molar, like the number of root canals; the number of roots may also vary. An additional third root, first mentioned in the literature by Carabelli[4] is called the radix entomolaris (RE) .This supernumerary root is located distolingually in mandibular molars, mainly first molars. An additional root at the mesiobuccal side is called the radix paramolaris.
Case Report
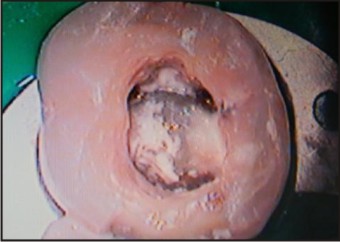
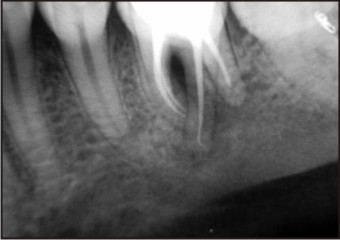
A 25 year male patient was reported to the Department of Conservative Dentistry and Endodontics, with a complaint of pain on chewing in right lower back tooth. On clinical examination there was deep class 1 caries in mandibular right first permanent molar (#46). Tooth (#46) showed negative response on vitality testing, and was tender on percussion. Intra oral periapical radiograph revealed the presence of peri-apical radiolucency around both mesial and distal roots (Fig 1). This radiograph also showed that the tooth had an additional distolingual root (Fig 1). Diagnosis of symptomatic apical periodontitis was made and root canal treatment was recommended. Local anesthesia (inferior alveolar nerve block) was performed. The tooth was isolated by a rubber dam, and then the access cavity was prepared with distolingual extension to provide proper access to distolingual canal (Fig 2). After finding orifices of the canal under microscope (Fig 3), a radiograph was taken to determine the working length of the canals with two instruments in mesial root and two instruments in the distal roots (Fig 4). Shaping and cleaning was performed using rotary pro-taper files (DENTSPLY, Maillefer, Swiss made CH-1338 Ballaigues) in crown down manner. Apical preparation was done till size F2 protaper file (master apical file). The canals were irrigated with 5.25% sodium hypochlorite, 0.2%w/v chlorhexidine gluconate (Vishal Dentocare Pvt, Ltd India) during instrumentation and finally with normal saline.
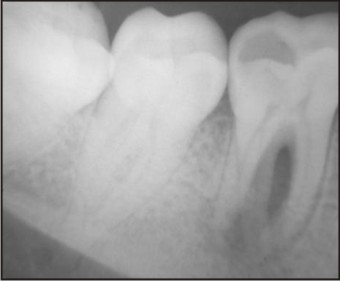 | Fig 1 : Preoperative Radiograph showing radiolucency involving mesial and distal roots of 46.
 |
 | Fig 2 : Clinical image of access cavity.
|
 | Fig 3 : Microscopic view of orifices location of radix entomolaris.
|
 | Fig 4 : Working length of 46
|
The canals were then dried with paper points, master cone selection radiograph was taken, and obturated with laterally condensed gutta percha (DENTSPLY, Maillefer, Swiss made CH-1338 Ballaigues) and AH plus sealer (DENTSPLY DeTrey GmbH, Germany). Post endodontic restoration was placed and patient was recalled for follow up and full coverage crown. (Fig 5 & 6).
 | Fig 5 : Orifices of obturated radix entomolaris 46.
|
 | Fig 6 : Post operative radiograph showing obturation of all the canals and post endodontic restoration.
|
Discussion
Etiology behind Radix
Etiology behind the formation of the RE is still unclear. In dysmorphic, supernumerary roots, its formation could be related to external factors during odontogenesis, or to penetrance of an atavistic gene or polygenetic system (atavism is the reappearance of a trait after several generations of absence). In eumorphic roots, racial genetic factors influence the more profound expression of a particular gene that results in the more pronounced phenotypic manifestation[5],[6]. Curzon suggested that the ‘three-rooted molar’ trait has a high degree of genetic penetrance as its dominance was reflected in the fact that the prevalence of the trait was similar in both pure Eskimo and Eskimo/ Caucasian mixes [7]
Structure of Radix entomolaris (RE)
Radix entomolaris (RE) is characterized by the presence of an additional distolingual root, with its coronal third completely or partially fixed to the distal root. The dimensions of the RE can vary from a short conical extension to a ‘mature’ root with normal length and root canal. In general, the RE is smaller than the distobuccal and mesial roots and can be separate from, or partially fused with, the other roots. A classification by Carlsen and Alexandersen[8] describes four different types of RE according to the location of the cervical part of the RE: types A, B, C and AC. Types A and B refer to a distally located cervical part of the RE with two normal and one normal distal root components, respectively. Type C refers to a mesially located cervical part, while type AC refers to a central location, between the distal and mesial root components. This classification allows for the identification of separate and nonseparate RE.
 |
|
 |
|
In the apical two thirds of the RE, a moderate to severe mesially or distally orientated inclination can be present.
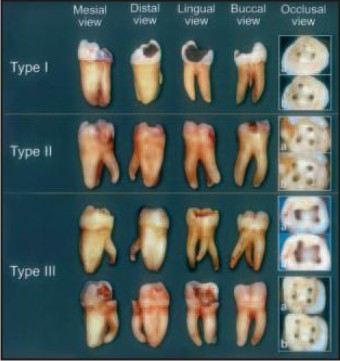
According to the classification[9], by De Moor et al based on the curvature of the separate RE variants in bucco-lingual orientation, three types can be identified-
Type I refers to a straight root/root canal.
Type II refers to an initially curved entrance which continues as a straight root/root canal.
Type III refers to an initial curve in the coronal third of the root canal and a second curve beginning in the middle and continuing to the apical third.
Endodontic Management
A thorough inspection of the preoperative radiograph and interpretation of particular marks or characteristics, such as an unclear view or outline of the distal root contour or the root canal, can indicate the presence of a ‘hidden’ RE. To reveal the RE, a second radiograph should be taken from a more mesial or distal angle (20 degrees)[10],[11],[12]. This way an accurate diagnosis can be made in the majority of cases. A dark line on the pulp chamber floor can indicate the precise location of the RE canal orifice. Apart from a radiographic diagnosis, clinical inspection of the tooth crown and analysis of the cervical morphology of the roots by means of periodontal probing can facilitate identification of an additional root. The location of the orifice of the root canal of an RE has implications for the opening cavity. The orifice of the RE is located distal- to mesiolingually from the main canal or canals in the distal root. An extension of the triangular opening cavity to the distolingual side results in a more rectangular or trapezoidal outline form. Visual aids such as a loupe, intra-oral camera or dental microscope can, in this respect, be useful.
There are various methods to locate additional canals,these are as follows-
1. Knowledge of law of symmetry and law of orificelocation.[13]
2. Tactile sensation with hand instrument
3. Using various instruments like endodontic explorer, pathfinder, DG 16 probe and mico-opener.
4. Champagne effect- bubbles produced by remaining pulp tissue in the canal, while using sodium hypochlorite in pulp chamber.
5. Introral periapical radiograph
6. Digital radiography
7. Using fiber-optic illumination dentaledoscopy andorascopy
8. Using surgical loupes
9. Using Operating microscope
10. Micro Computed Tomography
11. Visualization endograph using Ruddle’s solution
12. Magnetic Resonance Microscopy
Conclusion
Dentist should be aware of unusual root morphology in mandibular first molar. The initial diagnosis of RE can be done with the help of angled preoperative periapical radiographs to facilitate endodontic procedure and avoid missed canals. In the case of an RE the conventional triangular openin gcavity must be modified to a trapezoidal form in order to better locate and access the distolingually located orifice of the additional root. Knowledge of location of additional root canal orifice s and root canal curvature will result in successful endodontic outcome.
References
1. Barker BC, Parson KC, Mills PR, Williams GL. Anatomy of root canals. III. Permanent mandibular molars. Aust Dent J 1974; 19: 403–13.
2. Vertucci FJ. Root canal anatomy of the human permanent teeth.Oral Surg Oral Med Oral Pathol 1984; 58: 589 –99.
3. Jamileh Ghoddusi,Neda N aghavi, Mina Zarei and Ehsan Rohani. Mandibular first molar with four distal roots.J. Endo 2007;33;1481-1483.
4. Filip l. Calberson, Roeland J. De Moor, and Christophe A. Deroose. The Radix Entomolaris and Paramolaris: Clinical Approach in Endodontics. J Endod 2007; 33: 58–63
5. Reichart PA, Metah D. Three-rooted permanent mandibular first molars in the Thai. Community Dent Oral Epidemiol 1981;9:191–2.
6. Ribeiro FC, Consolaro A. Importancia clinicay antropologica de la raiz distolingual en los molars inferiors permanentes. Endodoncia 1997;15:72– 8.
7. Curzon ME. Miscegenation and the prevalence of three-rooted mandibular first molars in the Baffin Eskimo. Community Dent Oral Epidemiol 1974;2:130 –1.
8. Carlsen O, Alexandersen V. Radix entomolaris: identification and morphology. Scan J Dent Res 1990;98:363–73.
9. De Moor RJ, Deroose CA, Calberson FL. The radix entomolaris in mandibular first molars: an endodontic challenge. Int Endod J 2004;37:789 –99.
10. Ingle JI, Heithersay GS, Hartwell GR et al. (2002) Endodonticdiagnostic procedures. In: Ingle JI, Bakland LF, eds.Endodontics, 5th edn. Hamilton, London, UK: BC Decker Inc.,203–58
11. Walton RE (1973) Endodontic radiographic techniques. DentalRadiography and Photography 46, 51–9.
12. Goerig AC, Neaverth EJ (1987) A simplified look at the buccalobject rule in endodontics. J Endod 13, 570–2
13. Krasner P, Rankow H. Anatomy of pulp chamber fl oor. J Endod. 2003; 30(1):5-16.
|